
Abstract
Summary
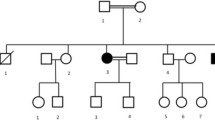
A new case of familial tumoral calcinosis (FTC)/hyperostosis–hyperphosphatemia syndrome (HHS) due to a novel compound heterozygous mutation in N-acetylgalactosaminyltransferase 3 (GALNT3) and with new phenotypic findings is presented. The response in serum phosphate and fibroblast growth factor 23 (FGF23) to medical treatment is detailed. This case expands the genotype and phenotype of FTC/HHS and gives insight into its treatment and pathophysiology.
Introduction
FTC and HHS are caused by mutations in FGF23, GALNT3, or KLOTHO. They are characterized by hyperphosphatemia, increased phosphate reabsorption, and elevated or inappropriately normal serum 1,25-dihydroxyvitamin D3 (1,25-D3); FTC is associated with calcific masses, and HHS with diaphyseal hyperostosis.
Methods
A 36-year-old woman presented with abnormal dental X-rays at age 12 and was hyperphosphatemic at 22. She underwent radiographic, biochemical and genetic testing, and medical treatment.
Results
Serum phosphorus was 7.3 mg/dL (2.5–4.8), TmP/GFR 6.99 mg/100 mL (2.97–4.45), 1,25-D3 35 pg/mL (22–67). Radiographs revealed tooth anomalies, thyroid cartilage calcification, calcific masses in vertebral spaces, calcification of the interstitial septa of the soft tissue in the lower extremities, and cortical thickening of the long bones. Her total hip Z score was 1.9. C-terminus serum FGF23 was 1,210 RU/mL (20–108), but intact FGF23 was 7.4 pg/mL (10–50). DNA sequencing determined she was a compound heterozygote for mutations in GALNT3. Treatment with niacinamide and acetazolamide decreased TmP/GFR and serum phosphate, which was paralleled by a decrease in serum C-terminus FGF23.
Conclusions
This case broadens the spectrum of phenotypic and genotypic features of FTC/HHS and suggests treatments to decrease renal phosphate reabsorption in the setting of a low intact FGF23.


Similar content being viewed by others


References
Benet-Pages A, Orlik P, Strom TM, Lorenz-Depiereux B (2004) An FGF23 missense mutation causes familial tumoral calcinosis with hyperphosphatemia. Hum Mol Genet 14(3):385–390
Topaz O, Shurman DL, Bergman R, Indelman M, Ratajczak P, Mizrachi M, Khamaysi Z, Behar D, Petronius D, Friedman V, Zelikovic I, Raimer S, Metzker A, Richard G, Sprecher E (2004) Mutations in GALNT3, encoding a protein involved in O-linked glycosylation, cause familial tumoral calcinosis. Nat Genet 36(6):579–581
Ichikawa S, Imel EA, Kreiter ML, Yu X, Mackenzie DS, Sorenson AH, Goetz R, Mohammadi M, White KE, Econs MJ (2007) A homozygous missense mutation in human KLOTHO causes severe tumoral calcinosis. J Clin Invest 117(9):2684–2691
Frishberg Y, Topaz O, Bergman R, Behar D, Fisher D, Gordon D, Richard G, Sprecher E (2005) Identification of a recurrent mutation in GALNT3 demonstrates that hyperostosis–hyperphosphatemia syndrome and familial tumoral calcinosis are allelic disorders. J Mol Med 83(1):33–38
Ichikawa S, Guigonis V, Imel EA, Courouble M, Heissat S, Henley JD, Sorenson AH, Petit B, Lienhardt A, Econs MJ (2007) Novel GALNT3 mutations causing hyperostosis–hyperphosphatemia syndrome result in low intact fibroblast growth factor 23 concentrations. J Clin Endocrinol Metab 92(5):1943–1947
Ichikawa S, Imel EA, Sorenson AH, Severe R, Knudson P, Harris GJ, Shaker JL, Econs MJ (2006) Tumoral calcinosis presenting with eyelid calcifications due to novel missense mutations in the glycosyl transferase domain of the GALNT3 gene. J Clin Endocrinol Metab 91(11):4472–4475
Ichikawa S, Lyles KW, Econs MJ (2005) A novel GALNT3 mutation in a pseudoautosomal dominant form of tumoral calcinosis: evidence that the disorder is autosomal recessive. J Clin Endocrinol Metab 90(4):2420–2423
Riminucci M, Collins MT, Fedarko NS, Cherman N, Corsi A, White KE, Waguespack S, Gupta A, Hannon T, Econs MJ, Bianco P, Gehron Robey P (2003) FGF-23 in fibrous dysplasia of bone and its relationship to renal phosphate wasting. J Clin Invest 112(5):683–692
Razzaque MS, Lanske B (2007) The emerging role of the fibroblast growth factor-23-klotho axis in renal regulation of phosphate homeostasis. J Endocrinol 194(1):1–10
Kato K, Jeanneau C, Tarp MA, Benet-Pages A, Lorenz-Depiereux B, Bennett EP, Mandel U, Strom TM, Clausen H (2006) Polypeptide GalNAc-transferase T3 and familial tumoral calcinosis. Secretion of fibroblast growth factor 23 requires O-glycosylation. J Biol Chem 281(27):18370–18377
Frishberg Y, Ito N, Rinat C, Yamazaki Y, Feinstein S, Urakawa I, Navon-Elkan P, Becker-Cohen R, Yamashita T, Araya K, Igarashi T, Fujita T, Fukumoto S (2007) Hyperostosis–hyperphosphatemia syndrome: a congenital disorder of O-glycosylation associated with augmented processing of fibroblast growth factor 23. J Bone Miner Res 22(2):235–242
Strewler GJ (2007) Untangling klotho’s role in calcium homeostasis. Cell Metab 6(2):93–95
Olauson H, Krajisnik T, Larsson C, Lindberg B, Larsson T (2008) A novel missense mutation in GALNT3 causing hyperostosis–hyperphosphatemia syndrome. Eur J Endocrinol 158:929–934
Jonsson KB, Zahradnik R, Larsson T, White KE, Sugimoto T, Imanishi Y, Yamamoto T, Hampson G, Koshiyama H, Ljunggren O, Oba K, Yang IM, Miyauchi A, Econs MJ, Lavigne J, Juppner H (2003) Fibroblast growth factor 23 in oncogenic osteomalacia and X-linked hypophosphatemia. N Engl J Med 348(17):1656–1663
The ADHR Consortium (2000) Autosomal dominant hypophosphataemic rickets is associated with mutations in FGF23. Nat Genet 26(3):345–348
Chefetz I, Heller R, Galli-Tsinopoulou A, Richard G, Wollnik B, Indelman M, Koerber F, Topaz O, Bergman R, Sprecher E, Schoenau E (2005) A novel homozygous missense mutation in FGF23 causes familial tumoral calcinosis associated with disseminated visceral calcification. Hum Genet 118(2):261–266
Burkes EJ Jr, Lyles KW, Dolan EA, Giammara B, Hanker J (1991) Dental lesions in tumoral calcinosis. J Oral Pathol Med 20(5):222–227
Specktor P, Cooper JG, Indelman M, Sprecher E (2006) Hyperphosphatemic familial tumoral calcinosis caused by a mutation in GALNT3 in a European kindred. J Hum Genet 51(5):487–490
Garringer HJ, Mortazavi SM, Esteghamat F, Malekpour M, Boztepe H, Tanakol R, Davis SI, White KE (2007) Two novel GALNT3 mutations in familial tumoral calcinosis. Am J Med Genet A 143A(20):2390–2396
Campbell PI, Abraham MI, Kempson SA (1989) Increased cAMP in proximal tubules is acute effect of nicotinamide analogues. Am J Physiol 257(6 Pt 2):F1021–F1026
Beck N, Kim KS, Wolak M, Davis BB (1975) Inhibition of carbonic anhydrase by parathyroid hormone and cyclic AMP in rat renal cortex in vitro. J Clin Invest 55(1):149–156
Yamaguchi T, Sugimoto T, Imai Y, Fukase M, Fujita T, Chihara K (1995) Successful treatment of hyperphosphatemic tumoral calcinosis with long-term acetazolamide. Bone 16(4 Suppl):247S–250S
Benet-Pages A, Lorenz-Depiereux B, Zischka H, White KE, Econs MJ, Strom TM (2004) FGF23 is processed by proprotein convertases but not by PHEX. Bone 35(2):455–462
Acknowledgments
This research was supported, in part, by the Intramural Research Program of the NIH, National Institute of Dental and Craniofacial Research. KEW and EGF are supported by NIH DK063934.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dumitrescu, C.E., Kelly, M.H., Khosravi, A. et al. A case of familial tumoral calcinosis/hyperostosis–hyperphosphatemia syndrome due to a compound heterozygous mutation in GALNT3 demonstrating new phenotypic features. Osteoporos Int 20, 1273–1278 (2009). https://doi.org/10.1007/s00198-008-0775-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-008-0775-z