
Abstract
Purpose
To evaluate the potential preventive effect of probiotics on ventilator-associated pneumonia (VAP).
Methods
This was an open-label, randomized, controlled multicenter trial involving 235 critically ill adult patients who were expected to receive mechanical ventilation for ≥48 h. The patients were randomized to receive (1) a probiotics capsule containing live Bacillus subtilis and Enterococcus faecalis (Medilac-S) 0.5 g three times daily through a nasogastric feeding tube plus standard preventive strategies or (2) standard preventive strategies alone, for a maximum of 14 days. The development of VAP was evaluated daily, and throat swabs and gastric aspirate were cultured at baseline and once or twice weekly thereafter.
Results
The incidence of microbiologically confirmed VAP in the probiotics group was significantly lower than that in the control patients (36.4 vs. 50.4 %, respectively; P = 0.031). The mean time to develop VAP was significantly longer in the probiotics group than in the control group (10.4 vs. 7.5 days, respectively; P = 0.022). The proportion of patients with acquisition of gastric colonization of potentially pathogenic microorganisms (PPMOs) was lower in the probiotics group (24 %) than the control group (44 %) (P = 0.004). However, the proportion of patients with eradication PPMO colonization on both sites of the oropharynx and stomach were not significantly different between the two groups. The administration of probiotics did not result in any improvement in the incidence of clinically suspected VAP, antimicrobial consumption, duration of mechanical ventilation, mortality and length of hospital stay.
Conclusion
Therapy with the probiotic bacteria B. Subtilis and E. faecalis are an effective and safe means for preventing VAP and the acquisition of PPMO colonization in the stomach.
Similar content being viewed by others


Introduction
Ventilator-associated pneumonia (VAP) in mechanically ventilated patients is the most commonly occurring nosocomial bacterial infection in the intensive care unit (ICU), with reported incidences as high as 78 % [1]. VAP is associated with prolonged hospital stay, increased medical costs and higher morbidity and mortality rates [1, 2]. Because VAP is largely preventable, strategies aimed at preventing/reducing the incidence of this infection is a major challenge to ICUs.
The pathogenesis of VAP usually requires two important processes: bacterial colonization of the upper digestive tract and aspiration of contaminated secretions into the lower airway. One therapeutic approach to prevent VAP which gained support is the implementation of measures aimed at attenuation of the burden of bacterial colonization in the upper digestive tract. Selective decontamination of the digestive tract using non-absorbable antibiotics topically applied to the gastrointestinal tract and systemic antibiotic prophylaxis has been reported to decrease the incidence of VAP [3, 4] and reduce mortality rates by eradicating microorganisms from the stomach. However, the constant threat of Gram-positive bacteria overgrowth and the development of antibiotic resistance in both Gram-positive and Gram-negative organisms, as well as the absence of any formal analysis of the impact of these effects on morbidity and mortality, have limited the widespread use of selective decontamination of the digestive tract [5, 6].
A promising alternative is to use probiotic bacteria which are defined as “living microorganisms that (when ingested) have a beneficial effect in the prevention and treatment of specific pathologic conditions” [7]. Probiotics have been proposed to exert beneficial effects by enhancing gut barrier function, inhibiting colonization of potentially pathogenic microorganisms (PPMOs), maintaining a normal intestinal milieu, synthesizing antibacterial substances and stimulating local immunity, among others [8, 9]. Probiotics may exert their preventive effect on VAP by reducing bacterial colonization in the upper digestive tract via a combination of local and systemic effects [10]. A pilot study reported that the number of mechanically ventilated patients with pathogenic enteric bacterial colonization of the oropharynx or trachea was lower when the patients received oral care involving the probiotic Lactobacillus plantarum 299 [11]. While it has not yet been proven that probiotics induce the selection and overgrowth of antibiotic-resistant microorganisms, it has been shown that probiotics do inhibit antibiotic-resistant bacteria colonizing in the digestive tract. Oral administration of probiotic yoghurt (containing Lactobacillus rhamnosus GG) was associated with a significant reduction in gastrointestinal carriage of vancomycin-resistant enterococci [12]. Moreover, probiotics have other critical advantages which antibiotics do not have, such as high safety and no obvious contraindication in clinical application. Therefore, we hypothesized that probiotics would reduce the incidence of VAP in patients receiving mechanical ventilation by reducing the colonization of PPMOs in the stomach and the oropharynx.
Methods
Patients
Patients admitted to any one of the 11 participating ICUs in nine Chinese teaching hospitals between May 2010 and April 2015 were consecutively screened for entry into this clinical trial. The ICUs served a mixed population of medical, surgical, trauma and neurologic patients.
All critically ill adult patients (age ≥18 years) with an expected need of mechanical ventilation for at least 48 h were eligible for entry into the study. Exclusion criteria were: (1) age of <18 years or >80 years; (2) severe multiple organ failure, with an Acute Physiology and Chronic Health Evaluation (APACHE) II score of ≥25; (3) mechanical ventilation for >72 h prior to enrollment; (4) failure of enteral feeding; (5) administration of immunodepressants 1 week before enrollment or diagnosis of immunosuppressive diseases, such as malignant tumor, acquired immune deficiency syndrome and human immunodeficiency virus carriers; (6) pregnancy or lactation. Informed written consent was obtained from each patient or a legal representative of the family. This study protocol was approved by the human ethics committees in Shandong University (protocol no. 2009021) and was carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association.
Study design
This clinical trial was designed as a prospective, open-label, randomized, controlled multicenter study. Patients meeting the inclusion criteria were enrolled and randomized (in a 1:1 ratio) into a probiotics group and a control group, respectively, within 24 h of admission to the ICU or within 24 h of tracheal intubation if the intubation occurred in the ICU. The probiotic group was given commercially available probiotics capsules (Medilac-S, China) 0.5 g three times daily plus standard preventive strategies of VAP, and the control group received standard preventive strategies only. Patients in the probiotics group started taking the capsules within 2 h after randomization. The standard preventive strategies of VAP included daily screening for weaning potential and weaning from mechanical ventilation as soon as possible, hand hygiene, aspiration precautions and prevention of contamination (the “WHAP” strategies) [13]. All patients were placed in a semi-recumbent position in the absence of contraindication. Continuous control of tracheal cuff pressure was maintained at around 25 cm H2O using a manometer to prevent regurgitation and aspiration. A tracheal tube which enabled subglottic secretion aspiration was the first choice and the preferred option over the normal tracheal tube. Until enteral feeding was established, all patients admitted to the ICU received intravenous proton pump inhibitors as stress ulcer prophylaxis. Enteral feeding was started as soon as possible when gastrointestinal peristalsis was present. Moreover, chest radiographs were performed on all patients after tracheal incubation and thereafter when clinically indicated; endotracheal suctioning was performed by the nursing staff if necessary. When mechanical ventilation was expected to be necessary for >3 weeks, patients received a tracheotomy. Normal oropharyngeal care measures included rinsing the mouth with water and, if possible, brushing the teeth once daily. To prevent cross-acquisition, dispensers filled with disinfectants were placed at each bedside, and the staff in ICU was regularly educated to comply with infection control procedures during the study period.
This study continued until tracheal extubation, discharge from the hospital or death, with a maximum study duration of 14 days. Each probiotics capsule contained active Bacillus subtilis and Enterococcus faecalis at a concentration of 4.5 × 109/0.25 g and 0.5 × 109/0.25 g, respectively. All patients had a nasogastric tube. For delivery to the patient, the probiotics capsules were first broken open and the contents diluted in 50–80 ml sterile water; this solution was administered as a bolus through a nasogastric tube by the nursing staff. All probiotics capsules were stored at 4 °C. Researchers checked each patient’s consumption and recorded missed or refused medications to assess compliance. A patient who took more than 80 % of the study medication was considered to be compliant.
Sample size
The incidence of VAP in China is approximately 60.0 % according to published data [14]. We estimated that a sample size of 234 patients (117 in each group) was required in order to have a power of 80 % to detect a difference of 20 % in the incidence of VAP between the control group and the probiotics group after treatment at a significance level of 5 % with an acceptable dropout rate (10 %).
Data collection
The age, sex, medical specialty, diagnosis at admission, reason for mechanical ventilation, prior antibiotic use, length of hospital stay before admission to ICU, and APACHE II scores (range 0–71, with higher scores indicating more severe illness) of each patient were recorded at baseline. The proportion of patients with a nasotracheal tube or tracheal tube with subglottic secretion drainage, who were started on early enteral nutrition (started within 48 h following ICU admission) and who used proton pump inhibitors during the study period were recorded. We also monitored prospectively the number of days studied, duration of mechanical ventilation, length of ICU and hospital stay, signs of infection (temperature, leukocyte counts and differential counts, interpretation of chest radiographs, microbiological results) and antibiotic use.
Ventilator-associated pneumonia
All patients were evaluated daily for the presence of VAP by the authors of the study. A clinical diagnosis of VAP was based on the presence of a new, persistent or progressive infiltrate on chest radiographs that persisted for at least 48 h (as interpreted by radiologists blinded to the patients’ treatment assignments) combined with at least two of the following criteria: (1) a temperature of >38.0 °C or <35.5 °C; (2) a blood leukocytosis count of >12 × 103/mm3 or <3 × 103/mm3 and/or left shift; (3) purulent tracheal aspirates [14, 15]. Prior to making a clinical diagnosis of VAP, the attending physician should exclude other pulmonary diseases such as acute respiratory distress syndrome, lung edema, pulmonary tuberculosis, pulmonary embolism, cryptogenic organizing pneumonia and acute interstitial pneumonia, among others. All clinical diagnoses of VAP were evaluated and agreed upon by two of the authors. Endotracheal aspirate samples for semiquantitative cultures of PPMOs were obtained from all patients with clinically diagnosed VAP. These cultures were scored using the four-quadrant method, with a score of 0 indicating no growth; 1+ = rare growth; 2+ = light growth; 3+ = moderate growth; 4+ = heavy growth. A score of 3+ or 4+ defined the presence of microbiologically confirmed VAP in the semiquantitative cultures of endotracheal aspirate. Early-onset VAP was defined as VAP diagnosed within the first 4 days of mechanical ventilation, and late-onset VAP was diagnosed when VAP presented thereafter. All members of the microbiology laboratory were blind to the study.
Microbiology
The throat swabs and gastric aspirate were sent to the microbiology laboratory for surveillance semi-quantitative culture of PPMOs at baseline and subsequently once or twice weekly. Bacteriological culture was performed using standard microbiological methods, and antibiotic susceptibility was evaluated by means of the Kirby–Bauer disk diffusion testing method according to the guidelines established by the National Committee for Clinical Laboratory Standards (NCCLS). The NCCLS criteria for susceptibility and resistance were used. Antibiotic-resistant bacteria were defined as Gram-negative bacteria resistant to aminoglycosides, third-generation cephalosporins, extended-spectrum penicillins, quinolones or imipenem, and Gram-positive bacteria were defined as those resistant to oxacillin or vancomycin. All members of the microbiology laboratory were blind to the study.
Definitions
Colonization at baseline, eradication of colonization and acquired colonization were defined as reported previously [16]. Colonization was defined as the presence of microorganisms in two or more consecutive specimens from one site without infection. Colonization at baseline was defined as colonization demonstrated before enrollment or within 24 h after enrollment. Eradication of colonization was defined as the absence of microorganisms in two or more consecutive cultures of one site that was colonized at baseline; this measure was reported as the proportion of colonized patients for whom eradication occurred. Acquired colonization was defined as colonization which occurred >24 h after enrollment in patients without colonization at baseline.
Data analysis
The primary endpoints of the study were the incidence of microbiologically confirmed VAP in patients intubated for ≥48 h and the proportions of eradication of colonization and acquired colonization with PPMOs in the oropharynx and stomach. The secondary endpoints were number of days on mechanical ventilation, of days in the ICU and of days in the hospital after ICU admission, mortality (in ICU, in hospital) and number of days of antibiotic use for VAP, of antibiotic-free days at day 28, of carbapenem-free days at day 28 and of glycopeptide- or linezolid-free days at day 28.
Statistical analysis
Categorical data were presented as proportions or percentages and analyzed by the Chi-square or Fisher exact test. Normality of all data sets was determined using the Kolmogorov–Smirnov test. Parametric data were expressed as mean ± standard deviation and analyzed by the two-tailed, paired or nonpaired t test, while nonparametric data were reported as medians with interquartile ranges and analyzed by the Mann–Whitney U test. Kaplan–Meier analyses with log rank tests were performed to calculate the probability of remaining without VAP. Incidence rates of pneumonia were compared by using risk ratios (RR) with 95 % confidence intervals (CI). The SPSS for Windows statistical program (version 12.0; IBM Corp., Armonk, NY) was used for data statistics. Statistical significance was set at P < 0.05 and highly significant values had a significance of P < 0.01.
Results and discussion
Study population
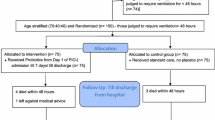
A total of 457 patients were screened, of whom 207 were excluded from entry to the study because of an expected need for mechanical ventilation of <48 h, refusal to give informed consent and exclusion criteria. The remaining 250 patients were randomly assigned to the probiotics group or to the control group. Following randomization, 15 patients did not complete the study; the remaining 235 patients did complete the study (Fig. 1). Probiotics capsules were administered to those patients in the probiotics group according to the study protocol on 95.8 % of all patient-days.

Flow diagram of patient enrollment
The demographic and baseline characteristics were similar between the two groups, as listed in Table 1. There were no significant differences between the study (probiotics) group and the control group terms of in APACHE II scores, proportions of patients with nasotracheal tube, proportions of patients with tracheal tube with subglottic secretion aspiration, antibiotic use on admission, initiation of early enteral feeding, prescription of proton pump inhibitors during the study and the length of time intubated before randomization.
Primary endpoints of the study
Ventilator-associated pneumonia
Among the 118 patients receiving the probiotics capsules containing live microorganisms, 43 (36.4 %) were diagnosed with microbiologically confirmed VAP, as compared with 59 of the 117 (50.4 %) patients in the control group (P = 0.031; Table 2). Although the incidence of clinically diagnosed VAP tended to be lower in probiotics patients (40.7 %) than in control patients (53.0 %), this difference was not statistically significant (P = 0.059; Table 2). The probability of remaining free of VAP during the study period was significantly higher in the probiotics group than in the control group (P = 0.004 by the log rank test) (Fig. 2). Compared to the control group, the administration of prophylactic probiotics resulted in a RR for VAP of 0.72 (95 % CI 0.53–0.97), which is a reduction in the RR of 0.28 (95 % CI 0.03–0.47) and a reduction in the absolute risk of 0.14 (95 % CI 0.0081–0.2719), indicating that seven patients need to be treated to prevent one episode of VAP. The mean time to the onset of VAP after tracheal intubation was significantly longer in the probiotics group than in the control group (10.4 vs. 7.5 days, respectively; P = 0.022).

The probability of remaining ventilator-associated pneumonia-free (VAP-free) during the study period in the probiotics and control groups
Approximately 20 % of the episodes of microbiologically confirmed VAP were early-onset episodes. The proportion of patients with late-onset VAP was similar in the probiotics group and control group (83.7 vs. 79.7 %, respectively; P = 0.603). The pathogens isolated from lower respiratory tract from patients with VAP are reported in Table 2. The most commonly isolated etiologic pathogens of VAP in both groups were Gram-negative organisms, of which the most common were Pseudomonas aeruginosa and Acinetobacter baumannii. The most commonly isolated Gram-positive microorganism in both groups was Staphylococcus aureus. There was no significant difference in the types of isolated pathogens between the probiotics group and the control group (P = 0.866) (Table 2). The number of recurrent episodes of VAP during the study period was very low in both the probiotics group and control group, possibly due to the relative short duration of the study period.
PPMO colonization of the oropharynx and stomach
The proportion of patients with colonization of PPMOs in the oropharynx at baseline was 27.1 % in the probiotics group and 23.9 % in the control group (P = 0.575). At baseline, PPMO colonization of the stomach was detected in 15.3 % of the patients in the probiotics group and 22.2 % the patients in the control group (P = 0.171) (Table 3). The colonization rates of PPMOs, including Enterobacteriaceae, glucose non-fermentative Gram-negative bacteria species, Enterococcus species, Staphylococcus aureus, Streptococcus species and Candida species in the oropharynx and stomach were comparable for the probiotics and control groups [see Electronic Supplementary Material (ESM) Table E1].
Neither the eradication of colonization with PPMOs [46.9 (probiotics patients) vs. 32.1 % ( control patients); P = 0.245] nor the acquisition of colonization with PPMOs [44.2 (probiotics patients) vs. 52.8 % (control patients); P = 0.254) were significantly improved in the oropharynx after the probiotics therapy compared to the control therapy (Table 3). In addition, although prophylactic administration of the probiotics capsules containing live microorganisms was associated with a tendency toward the prevention of acquisition with PPMOs in the stomach [24 (probiotics patients) vs. 44 % (control patients); P = 0.004], it did not improve the eradication of gastric colonization with PPMOs [27.8 (probiotics patients) vs. 19.2 % (control patients); P = 0.756] (Table 3). The acquired gastric colonization rates of Enterobacteriaceae, glucose non-fermentative Gram-negative bacteria species, Enterococcus species, Staphylococcus aureus, Streptococcus species and Candida species were not significantly different between the probiotics group and control group (P = 0.452; ESM Table E1).
Secondary endpoints of the study
The median number of days studied and duration of mechanical ventilation were not significantly different between the probiotics group and the control group (Table 4). The administration of probiotics did not shorten the duration of antibiotic use: the number of days for which antibiotics were prescribed for VAP and the number of antibiotic-free days at day 28, carbapenem-free days at day 28 and glycopeptide- or linezolid-free days at day 28 were comparable for the probiotics and control patients. The number of days in the ICU and in the hospital after ICU admission were also comparable for the probiotics and control patients (Table 4). Although ICU mortality tended to be higher among probiotics patients (12.7 %) as compared with control patients (7.7 %), this difference was not statistically significant (P = 0.207; Table 4), and the mortality in the hospital between the two groups was not significantly different [10.7 (probiotics patients) vs. 14.8 % (control patients); P = 0.369; Table 4).
Safety
The probiotics treatment was found to be safe among our critically ill patients. There were no reported adverse events and severe adverse events related to the probiotics capsule, as expected.
Probiotics have been proposed as an effective treatment for the prevention of nosocomial infections, including postoperative infections and respiratory infections. Here, we report the results of a multicenter, open-label, randomized, controlled study on the use of two strains of living probiotics (B. subtilis and E. faecalis) for the prevention of VAP. We found that the administration of these two viable probiotics as a capsule was associated with a reduction of VAP incidence and a delay of VAP occurrence after tracheal incubation.
Five other randomized controlled clinical trials have also reported that probiotics therapy was associated with a statistically significant lower incidence of VAP compared with the control group, consistent with our results [15, 17–20]. In contrast, however, six different randomized controlled clinical trials [11, 21–25] have reported that the administration of probiotics was unable to prevent the occurrence of VAP. We suggest here a number of possible explanations for this disparity in results.
First, the study population was different in each study. Among the five clinical trials which found that probiotics had a preventive effect on VAP, there are three trials which included multiple trauma patients and one trial which included pediatric patients. The results of these trials were consistent with those of previous studies suggesting that trauma, surgical and pediatric patients may benefit from probiotics in terms of preventing various infections [26–28]. The study populations in the clinical trials which did not demonstrate any preventive effect of probiotics on VAP comprised critically ill patients on mechanical ventilation. Although our study also included mechanically ventilated ICU patients, in contrast to these other studies, we excluded those patients who had received mechanical ventilation for >72 h prior to enrollment. In addition, the maximum study period was 14 days. Consequently, our study population did not comprise ICU patients with prolonged mechanical ventilation which has been defined as a period of ≥21 days [29].
Secondly, a variety of definitions have been proposed to identify VAP and, consequently, the diagnostic criteria of VAP varied dramatically among all of the above-mentioned clinical trials. Vincent et al. reported that the incidence of VAP ranged from 4 to 42 % depending on which of six different diagnostic criteria they applied and that the delay before a diagnosis of VAP increased from 4 to 8 days with increasingly stringent criteria [30]. The incidence of VAP diagnosed with the same microbiological criteria as used in our study was 47 %, as previously reported [31], which is consistent with our results (50.4 % in the control group). A different meta-analysis with the aim to explore the potential benefits of probiotics on VAP prevention demonstrated that the pooled relative risk was higher when the clinical diagnostic criteria of VAP were used than when there was a microbiologically confirmed diagnosis [32]. Therefore, it is reasonable to assume that the different diagnostic criteria of VAP adopted in these different trials may have influenced the final results.
Thirdly, it should be realized that the clinical trials conducted to date have used different (combinations of) probiotic strains, dosing and administration route. There is a growing body of evidence in support of different strains of probiotics being able to exert their beneficial effects by multiple mechanisms and that the effects may vary with strain and study population. Previous studies which have proven the beneficial effect of probiotics on VAP prevention used a synbiotic formulation (Synbiotic 2000 Forte; prebiotic and probiotic combinations) or L. rhamnosus GG, but as these probiotic strains are not widely commercially available in China, we chose the widely used probiotics capsule Medilac-S. Furthermore, we chose two strains of living probiotics—and not a single probiotic strain—because probiotics exert their beneficial effect on multifactorial diseases, with a variety of probiotic properties, and such properties may be strain-specific [33]. When administered as a combination of strains, probiotics may complement each other and thus have synergistic probiotic effects.
Fourth, the design and sample size of these clinical trials varied widely. Only six trials were double-blind, and most were single-center. Among the clinical trials conducted to date which have found that probiotics could prevent VAP, our study is the only one with a sample size of >200 patients. However, there are three studies with a sample size of >200 patients among the clinical trials which found that probiotics could not prevent VAP. It is possible that the sample size could have influenced the observed incidence of VAP in the above-mentioned studies on VAP prevention, as has been reported [34].
The potential mechanisms by which probiotics therapy exerts its preventative effect on VAP are based on the possibility that probiotics are able to re-establish the normal balance of gastrointestinal microflora during medical interventions in critically ill patients. In our clinical trial, there was decreased acquisition of PPMO colonization in the stomach—but not in the oropharynx—in the probiotics group as compared with the control group. Furthermore, there was no significant difference between the probiotics and control groups with regards to the eradication of colonization by PPMOs in the stomach or the oropharynx. These data indicate that the probiotics administered to our patients were able to prevent gastric colonization by PPMOs, but they could not eradicate the colonization of gastric PPMOs in mechanically ventilated ICU patients. Consistent with our study, Jain and colleagues demonstrated in a randomized, placebo-controlled study that compared with the controls, septic patients treated with synbiotic preparations (Lactobacillus acidophilus, Bifidobacterium lactis, Streptococcus thermophilus and Lactobacillus bulgaricus with oligofructose) had a significantly lower incidence of PPMOs (43 vs. 75 %; P = 0.05) and multiple organisms (39 vs. 75 %; P = 0.01) in their nasogastric aspirates [35]. Morrow et al. [15] also showed that the administration of the probiotic Lactobacillus rhamnosus GG to critically ill patients at high risk of developing VAP significantly reduced the rates of gastric colonization with pathogenic species than placebo.
One interesting finding of our study was that although the probiotics therapy was associated with a reduced incidence of VAP and a delayed occurrence of VAP, there were no significant differences between the two groups in terms of mortality, duration of mechanical ventilation and antibiotic consumption, a result which is consistent with previously reported data [18, 19]. Many other evolving factors other than VAP, such as organ failure, may contribute to the death of critically ill patients. A possible explanation of our finding is that mortality attributable to VAP is likely to be much lower than initially believed, as suggested by Bekaert et al. [36] who reappraised attributable mortality of VAP and found that only 4.4 % of the deaths at 30 days and 5.9 % of those at 60 days could be attributable to VAP. Similarly, other complications which develop during the ICU stay, such as muscle weakness, pressure ulcer, pulmonary embolism and hyperactive delirium, also increase the duration of mechanical ventilation [37]. In our study, the incidence of clinically diagnosed VAP was comparable in the two groups (P = 0.059), and the physicians initiated antibiotic treatment for VAP and stopped antibiotic use according to the clinical signs—but not microbiological data. So although probiotics was associated with the reduced incidence of VAP, the consumption of antibiotics for VAP did not decrease accordingly. The preventive effect of probiotics on other types of nosocomial infections, such as urinary tract infection and (catheter-related) bloodstream infection, among others, is beyond the scope of our study and may explain why broad-spectrum antimicrobial use did not decrease accordingly. However, although the probiotics therapy did not improve the outcomes of the ICU patients, it does not mean that the prevention of VAP should be abandoned. According to Bekaert et al. [36], about 1 in 20 deaths in ICU might be avoided if all development of VAP could be prevented. Since VAP is largely preventable, any effort to prevent VAP remains worthwhile.
Several limitations to our study must be addressed. First, this study was an open-label study, which may affect a patient’s outcome and the investigators’ management. However, the clinical diagnosis of VAP was evaluated and agreed upon by two of the authors, and other outcomes collected, such as bacteria culture results, length of stay, etc., were objective data; both factors could minimize the observer bias. Secondly, we excluded those patients with mechanical ventilation for >72 h before enrollment and the maximum of the study period was 14 days; as such, the study population comprised patients with non-prolonged mechanical ventilation, and the results can not be generalized to the general ICU ventilated population. Thirdly, we did not use quantitative cultures with invasive samples as the microbiological VAP criteria for the following reasons: (1) semi-quantitative cultures correlate well with quantitative cultures for VAP diagnosis [38]; (2) quantitative cultures with invasive samples are associated with a number of limitations, such as low reproducibility [39]; (3) invasive samples taken by bronchoscopy may be subject to operator- and/or center-dependent variability which may affect the results; (4) there is no evidence that the use of quantitative cultures or invasive methods could improve the outcomes in patients with VAP [40]. Fourthly, this study was designed as a pilot trial and the sample size was relatively small. Further well-designed studies with large sample size will be needed to evaluate the preventive effect of probiotics on occurrence of VAP.
Conclusions
Our data suggest that treatment with a combination of live probiotics (B. subtilis and E. faecalis) is effective and safe in terms of preventing VAP in ICU patients with non-prolonged mechanical ventilation. The underlying mechanism involves prevention of the acquisition of PPMO colonization in the stomach. The data from this study justifies further study of probiotics for the prevention of VAP and its effect on gastrointestinal colonization of PPMOs.
References
Rello J, Ollendorf DA, Oster G, Vera-Llonch M, Bellm L, Redman R et al (2002) Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest 122:2115–2121. doi:10.1378/chest.122.6.2115
Safdar N, Dezfulian C, Collard HR, Saint S (2005) Clinical and economic consequences of ventilator-associated pneumonia: a systematic review. Crit Care Med 33:2184–2193. doi:10.1097/01.CCM.0000181731.53912.D9
de Smet AM, Kluytmans JA, Cooper BS, Mascini EM, Benus RF, van der Werf TS et al (2009) Decontamination of the digestive tract and oropharynx in ICU patients. N Engl J Med 360:20–31. doi:10.1056/NEJMoa0800394
de Jonge E, Schultz MJ, Spanjaard L, Bossuyt PM, Vroom MB, Dankert J et al (2003) Effects of selective decontamination of the digestive tract on mortality and acquisition of resistant bacteria in intensive care: a randomised controlled trial. Lancet 362:1011–1016. doi:10.1016/S0140-6736(03)14409-1
Lingnau W, Berger J, Javorsky F, Fille M, Allerberger F, Benzer H (1998) Changing bacterial ecology during a five-year period of selective intestinal decontamination. J Hosp Infect 39:195–206. doi:10.1016/S0195-6701(98)90258-4
Ebner W, Kropec-Hübner A, Daschner FD (2000) Bacterial resistance and overgrowth due to selective decontamination of the digestive tract. Eur J Clin Microbiol Infect Dis 19:243–247. doi:10.1007/s100960050470
Lilly DM, Stillwell RH (1965) Probiotics: growth promoting factors produced by microorganisms. Science 147:747–748. doi:10.1126/science.147.3659.747
Zeng J, Li YQ, Zuo XL, Zhen YB, Yang J, Liu CH (2008) Clinical trial: effect of active lactic acid bacteria on mucosal barrier function in patients with diarrhoea-predominant irritable bowel syndrome. Aliment Pharmacol Ther 28:994–1002. doi:10.1111/j.1365-2036.2008.03818.x
Gill HS, Guarner F (2004) Probiotics and human health: a clinical perspective. Postgrad Med J 80:516–526. doi:10.1136/pgmj.2003.008664
Jacobi CA, Schulz C, Malfertheiner P (2011) Treating critically ill patients with probiotics: beneficial or dangerous? Gut Pathogens 3:2. doi:10.1186/1757-4749-3-2
Klarin B, Molin G, Jeppsson B, Larsson A (2008) Use of the probiotic Lactobacillus plantarum 299 to reduce pathogenic bacteria in the oropharynx of intubated patients: a randomised controlled open pilot study. Crit Care 12:R136. doi:10.1186/cc7109
Manley KJ, Fraenkel MB, Mayall BC, Power DA (2007) Probiotic treatment of vancomycin-resistant enterococci: a randomised controlled trial. Med J Aust 186:454–457
Schultz MJ, Juffermans NP (2010) Prevention of VAP: “WHAP” should we do? Crit Care Med 38:706–707. doi:10.1097/CCM.0b013e3181bfea4b
Chinese Society of Critical Care Medicine (2013) The guidelines for prevention, diagnosis and treatment of ventilator-associated pneumonia (2013). Zhonghua Nei Ke Za Zhi 52:524–543. doi:10.3760/cma.j.issn.0578-1426.2013.06.024
Morrow LE, Kollef MH, Casale TB (2010) Probiotic prophylaxis of ventilator-associated pneumonia: a blinded, randomized, controlled trial. Am J Respir Crit Care Med 182:1058–1064. doi:10.1164/rccm.200912-1853OC
Bergmans DCJJ, Bonten MJM, Gaillard CA, Paling JC, van der Geest S, van Tiel FH et al (2001) Prevention of ventilator-associated pneumonia by oral decontamination: a prospective, randomized, double-blind, placebo-controlled study. Am J Respir Crit Care Med 164:382–388. doi:10.1164/ajrccm.164.3.2005003
Giamarellos-Bourboulis EJ, Bengmark S, Kanellakopoulou K, Kotzampassi K (2009) Pro- and synbiotics to control inflammation and infection in patients with multiple injuries. J Trauma 67:815–821. doi:10.1097/TA.0b013e31819d979e
Kotzampassi K, Giamarellos-Bourboulis EJ, Voudouris A, Kazamias P, Eleftheriadis E (2006) Benefits of a synbiotic formula (Synbiotic 2000Forte) in critically ill trauma patients: early results of a randomized controlled trial. World J Surg 30:1848–18455. doi:10.1007/s00268-005-0653-1
Spindler-Vesel A, Benkgmark S, Vovk I, Cerovic O, Kompan L (2007) Synbiotics, prebiotics, glutamine, or peptide in early enteral nutrition: a randomized study in trauma patients. J Parenter Enteral Nutr 31:119–126. doi:10.1177/0148607107031002119
Banupriya B, Biswal N, Srinivasaraghavan R, Narayanan P, Mandal J (2015) Probiotic prophylaxis to prevent ventilator associated pneumonia (VAP) in children on mechanical ventilation: an open-label randomized controlled trial. Intensive Care Med 41:677–685. doi:10.1007/s00134-015-3694-4
Forestier C, Guelon D, Cluytens V, Gillart T, Sirot J, De Champs C (2008) Oral probiotic and prevention of Pseudomonas aeruginosa infections: a randomized, double-blind, placebo controlled pilot study in intensive care unit patients. Crit Care 12:R69. doi:10.1186/cc6907
Knight DJ, Gardiner D, Banks A, Snape SE, Weston VC, Bengmark S et al (2009) Effect of synbiotic therapy on the incidence of ventilator associated pneumonia in critically ill patients: a randomised, double-blind, placebo controlled trial. Intensive Care Med 35:854–861. doi:10.1007/s00134-008-1368-1
Barraud D, Blard C, Hein F, Marçon O, Cravoisy A, Nace L et al (2010) Probiotics in the critically ill patient: a double blind, randomized, placebo-controlled trial. Intensive Care Med 36:1540–1547. doi:10.1007/s00134-010-1927-0
Oudhuis GJ, Bergmans DC, Dormans T, Zwaveling JH, Kessels A, Prins MH et al (2011) Probiotics versus antibiotic decontamination of the digestive tract: infection and mortality. Intensive Care Med 37:110–117. doi:10.1007/s00134-010-2002-6
[No authors listed] (2015) Randomized controlled study of probiotics containing Lactobacillus casei (Shirota strain) for prevention of ventilator-associated pneumonia. J Med Assoc Thai 98:253–259
Sommacal HM, Bersch VP, Vitola SP, Osvaldt AB (2015) Perioperative synbiotics decrease postoperative complications in periampullary neoplasms: a randomized, double-blind clinical trial. Nutr Cancer 67:457–462. doi:10.1080/01635581.2015.1004734
Falcão de Arruda IS, de Aguilar-Nascimento JE (2004) Benefits of early enteral nutrition with glutamine and probiotics in brain injury patients. Clin Sci (Lond) 106:287–292. doi:10.1042/CS20030251
de Araujo GV, de Oliveira Junior MH, Peixoto DM, Sarinho ES (2015) Probiotics for the treatment of upper and lower respiratory-tract infections in children: systematic review based on randomized clinical trials. J Pediatr (Rio J). 91:413–427. doi:10.1016/j.jped.2015.03.002
Lone NI, Walsh TS (2011) Prolonged mechanical ventilation in critically ill patients: epidemiology, outcomes and modelling the potential cost consequences of establishing a regional weaning unit. Crit Care 15:R102. doi:10.1186/cc10117
Ego A, Preiser JC, Vincent JL (2015) Impact of diagnostic criteria on the incidence of ventilator-associated pneumonia. Chest 147:347–355. doi:10.1378/chest.14-0610
Scholte JB, van Dessel HA, Linssen CF, Bergmans DC, Savelkoul PH, Roekaerts PM et al (2014) Endotracheal aspirate and bronchoalveolar lavage fluid analysis: interchangeable diagnostic modalities in suspected ventilator-associated pneumonia? J Clin Microbiol 52:3597–3604. doi:10.1128/JCM.01494-14
Wang J, Liu KX, Ariani F, Tao LL, Zhang J, Qu JM (2013) Probiotics for preventing ventilator-associated pneumonia: a systematic review and meta-analysis of high-quality randomized controlled trials. PLoS One 8:e83934. doi:10.1371/journal.pone.0083934
Luyer MD, Buurman WA, Hadfoune M, Speelmans G, Knol J, Jacobs JA et al (2005) Strain-specific effects of probiotics on gut barrier integrity following hemorrhagic shock. Infect Immun 73:3686–3692. doi:10.1128/IAI.73.6.3686-3692.2005
Hurley JC (2008) Profound effect of study design factors on ventilator-associated pneumonia incidence of prevention studies: benchmarking the literature experience. J Antimicrob Chemother 61:1154–1161. doi:10.1093/jac/dkn086
Jain PK, McNaught CE, Anderson AD, MacFie J, Mitchell CJ (2004) Influence of synbiotic containing Lactobacillus acidophilus La5, Bifidobacterium lactis Bb 12, Streptococcus thermophilus, Lactobacillus bulgaricus and oligofructose on gut barrier function and sepsis in critically ill patients: a randomised controlled trial. Clin Nutr 23:467–475. doi:10.1016/j.clnu.2003.12.002
Bekaert M, Timsit JF, Vansteelandt S, Depuydt P, Vésin A, Garrouste-Orgeas M et al (2011) Attributable mortality of ventilator-associated pneumonia: a reappraisal using causal analysis. Am J Respir Crit Care Med 184:1133–1139. doi:10.1164/rccm.201105-0867OC
Loss SH, de Oliveira RP, Maccari JG, Savi A, Boniatti MM, Hetzel MP et al (2015) The reality of patients requiring prolonged mechanical ventilation: a multicenter study. Rev Bras Ter Intensiva 27:26–35. doi:10.5935/0103-507X.20150006
Hashimoto S, Shime N (2013) Evaluation of semi-quantitative scoring of Gram staining or semi-quantitative culture for the diagnosis of ventilator-associated pneumonia: a retrospective comparison with quantitative culture. J Intensive Care 1:2. doi:10.1186/2052-0492-1-2
Niederman MS (2010) The argument against using quantitative cultures in clinical trials and for the management of ventilator-associated pneumonia. Clin Infect Dis 51[Suppl 1]:S93–S99. doi:10.1086/653055
Berton DC, Kalil AC, Teixeira PJ (2014) Quantitative versus qualitative cultures of respiratory secretions for clinical outcomes in patients with ventilator-associated pneumonia. Cochrane Database Syst Rev 10:006482. doi:10.1002/14651858.CD006482.pub4
Acknowledgments
We thank Man Chen, Xin Qu, and Guo-qiang Qie from the Intensive Care Unit, Shandong Provincial Hospital affiliated to Shandong University, People’s Republic of China for advice and copy-editing. This clinical trial was funded by grants from the Specific Fund of Clinical Medical Research of the Chinese Medical Association (No: 10030180240) and from the National Natural Science Foundation of China (No: 81200238).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
All authors declare that they have no conflict of interest regarding the submission and publication of the work reported here.
Additional information
This clinical trial is registered at http://www.chictr.org.cn (ChiCTR-TRC-11001713).
Take home message: The administration of probiotics was associated with a reduction of VAP incidence and a delay of VAP occurrence after tracheal incubation. Probiotics treatment may have prevented gastric colonization with PPMOs, but it was unable to eradicate PPMO colonization in the stomach of mechanically ventilated ICU patients.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Zeng, J., Wang, CT., Zhang, FS. et al. Effect of probiotics on the incidence of ventilator-associated pneumonia in critically ill patients: a randomized controlled multicenter trial. Intensive Care Med 42, 1018–1028 (2016). https://doi.org/10.1007/s00134-016-4303-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-016-4303-x