
Abstract
Objectives
To improve the cross-correlation method for noninvasive, continuous monitoring of cerebral autoregulation, to evaluate this method in humans with intact and impaired autoregulatory capacity, and to compare it to the cuff deflation test.
Design and setting
Prospective study in the intensive care unit of a university hospital.
Patients and participants
Fourteen patients with severe head injury, six patients with subarachnoid hemorrhage, and nine healthy volunteers.
Interventions and measurements
Middle cerebral artery flow velocities and arterial blood pressure were monitored continuously. Aaslid's thigh cuff tests were performed and results were scored using Tiecks' model for autoregulation index. Data were then collected without any patient manipulation. The mean time delay between slow spontaneous oscillations of blood pressure and middle cerebral artery flow velocity was calculated by cross-correlation analysis. Data are expressed as median (lower/upper quartile).
Results
Healthy subjects had a higher autoregulation index than patients, 5.0 (5.0/5.5) vs. 3.3 (2.0/4.5). Slow oscillations of blood pressure and middle cerebral artery flow velocity showed a time delay of –2.0 s (–2.7/–1.7) in healthy subjects but were almost synchronal in patients, –0.07 s (–0.5/0.45). Inter-method agreement in diagnosing an intact or impaired cerebral autoregulation was obtained in 108 of 147 examinations of autoregulation (73.5%) and was considered moderate.
Conclusions
Cross-correlation analysis may serve as a simple, noninvasive, and continuous measure of cerebral autoregulation. The time delay of –2.0 s in healthy subjects is in good agreement with other studies. Short-term autoregulation tests and monitoring techniques based on slow spontaneous oscillations should not be used interchangeably.
Similar content being viewed by others


Introduction
Cerebrovascular autoregulation is a cerebral control mechanism adjusting cerebral vasomotor tone in response to changes in cerebral perfusion pressure to ensure a relatively constant cerebral blood flow [1]. Under conditions of severe traumatic brain injury and high-grade subarachnoid hemorrhage this intrinsic protective mechanism is frequently compromised [2, 3], suggesting that in these situations cerebral perfusion is critically dependent on cerebral perfusion pressure and consequently on therapeutic intervention. A reliable method that allows continuous monitoring of cerebral autoregulation would allow guiding cerebral perfusion pressure management, potentially improving outcome and decreasing morbidity [4, 5, 6].
Conventional cerebral autoregulation tests are based on a challenge of cerebral perfusion pressure and assessment of the response of middle cerebral artery blood flow velocity (FVMCA) as a noninvasive measure of changes in cerebral blood flow [7, 8]. The challenge can be induced pharmacologically or by special maneuvers, such as rapid thigh cuff release [9, 10], brief compression of the common carotid artery [11], and Valsalva's maneuver [12]. However, conventional autoregulation tests are time-consuming, require a critical manipulation of cerebral perfusion pressure, and are not suitable for continuous analyses.
Assuming that spontaneous or respiration-induced fluctuations in arterial blood pressure (ABP) are sufficient to induce cerebral perfusion pressure changes triggering an autoregulatory response, recent approaches applied signal analyses between ABP and FVMCA signals [12, 13]. This led to understanding of cerebral autoregulation as a high-pass filter model: the influence of low frequency oscillations of ABP on FVMCA are attenuated and delayed while fluctuations in the high frequency range remain uncontrolled [14, 15, 16]. Thus it should be possible to measure cerebral autoregulation by analyzing the time delay between slow oscillations of ABP and FVMCA. Cross-correlation analysis can explore the temporal relationship between two time series and has shown the ability to provide a continuous measure of cerebral autoregulation [17, 18].
The first aim of this study was to improve the cross-correlation method in terms of applicability and reliability for continuous measurement of cerebral autoregulation. Our second aim was to evaluate this improved cross-correlation approach in patients with severe traumatic brain injury and subarachnoid hemorrhage by comparing the measurements obtained with this method to results obtained using the thigh cuff method. The third aim was to assess intermethod agreement in diagnosing an intact or impaired cerebral autoregulation. These data were presented in poster form at the 17th Annual Congress of the ESICM, Berlin, 10–13 October 2004, and have been published in abstract form [19].
Subjects and methods
The study protocol was approved by the local ethics committee of the Medical College of the University Hospital of Dresden (EK188122000). Written informed consent for participation in this study was obtained from the patients' relatives.
Patients
We included 20 comatose patients (14 men, 6 women) with a median age of 42 years (range 18–77). Fourteen patients had severe traumatic brain injury (initial Glasgow Coma Scale 3–8), and six had severe subarachnoid hemorrhage (Hunt-Hess grade 3–5). Individual patient characteristics are provided in Table 1. All patients received an intracranial pressure monitoring device, either intraparenchymal (Codman MicroSensor Basic Kit) or intraventricular (External Drainage System II, both Codman Sàrl, Le Locle, Switzerland) within the first hours of hospital admission. Intracranial mass lesions were evacuated within the same initial neurosurgical procedure. General clinical management included continuous administration of midazolam and fentanyl for sedation and analgesia. The patient's upper body was elevated by 15–30°degrees. Volume-controlled mechanical ventilation was adjusted to achieve normoventilation by repeated arterial blood gas analysis. Cerebral perfusion pressure was actively maintained above 70 mmHg by administration of crystalloids, colloids, and vasopressors (norepinephrine). If intracranial pressure exceeded 20 mmHg, a bolus of osmodiuretics (mannitol) was administered (after the external ventricular drain had been opened).
Protocol
Our experimental protocol called for autoregulation measurements every 12 h provided that the patients were available and had not developed vasospasm (defined as FVMCA above 160 cm/s [20]) or intracranial hypertension greater than 25 mmHg. FVMCA was measured simultaneously using two transcranial Doppler flow velocity meter probes (2 MHz, DWL, MultiDopT2, Singen, Germany), fixed around the head by a flexible holder frame. Continuous ABP was measured via the radial artery using a standard arterial catheter (Vygon, Ecouen, France). Just before starting with autoregulation measurements arterial partial pressure of CO2 was determined. Three sequential thigh cuff tests (see below) were followed by data recording of 20 min for cross-correlation analysis. Before each of the recordings approx. 3 min was allowed for stabilization of baseline values. During the recording period all physiological parameters were carefully observed. No manipulations such as nursing, blood sampling or physiotherapy were allowed and ventilator settings were not changed just before or during testing.
A total of 105 (88 bilateral and 17 unilateral) measurements were performed in the 20 patients within a median monitoring period of 3.5 days (range 1–15). In 17 recordings only unilateral data were obtained, for reasons such as a broken Doppler transducer, an insufficient transtemporal window or problems with fixing the holder probe. Therefore the middle cerebral artery supplied territories were studied in total 193 times (in 20 patients).
Determination of cerebral autoregulation using the cuff deflation test
The cuff deflation test was applied as described by Aaslid et al. [10]. Briefly, this involved placement of thigh cuffs inflated to 20 mmHg above systolic blood pressure for 2 min, followed by rapid and simultaneous deflation resulting in a transient decrease in ABP and FVMCA. From the time course of ABP and FVMCA recovery the Doppler system automatically calculated a dynamic cerebral autoregulatory index (ARI). This index grades autoregulatory performance, reaching from 0 (absent autoregulation) to 9 (best autoregulation). Full details of the mathematical equations have been described elsewhere [9]. As recommended by Mahony et al. [21], three measurements were performed in each subject and averaged to obtain a mean ARI for each hemisphere.
Healthy subjects
For comparison with our patient group we also investigated nine healthy volunteers (four men, five women) with a median age of 26 years (range 14–30). None had a history or signs of cerebrovascular or cardiovascular disease. All test procedures were similar to those described for the patients except for ABP monitoring for which we used a noninvasive continuous approach (the servocontrolled infrared finger plethysmograph (Finapres 2300, Ohmeda, Englewood, Col., USA). The recordings were started after a resting period of 10 min to allow the subjects to become accustomed to the setting. In one control subject we did not obtain a continuous 10-min artifact-free recording for cross-correlation analysis; therefore cross-correlation results are presented for eight healthy volunteers. In some cases ARI could not be calculated for all three subsequent tests because of poor Finapres signals or artifacts (three cycles in one patient, two cycles in six patients, and one cycle in two patients).
Data acquisition and preprocessing
First, analogue ABP and FVMCA recordings were filtered by an analogue low-pass filter (Bessel, 10th order, 3 dB cutoff frequency 45 Hz). The data were then converted from analog to digital at 300 Hz using an 8-channel, 12-bit resolution DAQ 700 PCMCIA-card (National Instruments, Austin, Tex., USA). They were visualized and stored in a HP OmniBook XE3 notebook computer with a 900 MHz PentiumIII processor (Hewlett-Packard, Cupertino, Calif., USA) and resampled at 75 Hz (“raw signals”). A specially designed software program based on LabVIEW 7.0 (National Instruments) and MatLab 6.5 (MathWorks, Natick, Mass., USA) was used for data acquisition and further data processing. The ABP and FVMCA tracings were visually inspected to make sure that they were free of artifacts.
Cross-correlation analysis
The cross-correlation function provides a time delay τ and the correlation coefficient Rxy between periodic oscillations of two signals. Since slow spontaneous oscillations occur in the low frequency range of the spectrum [22, 23], the ABP and FVMCA signals were subjected to a 10th order Butterworth digital filter with a low-pass cutoff frequency of 0.1 Hz. The subsequent signal analysis was performed within moving time windows of 3 min, each overlapping 30 s, and the mean was removed in each 3-min window. We used only data segments presenting coherence of 0.6 between the signals at least at one given frequency. Then the software program calculated the normalized cross-correlation function for each pair of ABP and FVMCA signal segments. The positive maximum of the function was used to derive the time delay τ. Only positive maxima of correlation coefficients (Rxy) greater than 0.3 and cross-correlation time shifts within ±20 s were considered. Slow rhythmic ABP oscillations with amplitudes greater than 3% of the mean value of ABP during the moving window were considered large enough to trigger an autoregulatory response. The results of a 10-min recording period were included only if at least 24% of the analyzed data segments fulfilled all of the criteria mentioned above. The criteria for valid time delays were fulfilled in 132 of 193 (68.4%) measurements, and thus 132 middle cerebral artery territories in 19 patients remained for the final cross-correlation analysis.
Statistical analysis
Data are expressed as median (lower/upper quartile), unless otherwise specified. Differences between controls and patients were compared by the Mann-Whitney U test. The p value of 0.01 or less was accepted as statistically significant. Cohen's κ (calculating agreement beyond that expected by chance) was computed for varying cutoff points (10 equidistant cutoff points between minimum and maximum for each method, 100 dichotomizations in all). The cutoff points leading to the highest concordance (maximum κ) between methods were used to determine intermethod agreement in diagnosing an intact or impaired cerebral autoregulation. A κ value of 1 indicates perfect agreement, while a κ value of 0 indicates agreement equivalent to chance. Values for the κ coefficient were interpreted according to Landis and Koch [24].
Results
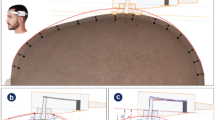
Physiological parameters (ABP, cerebral perfusion pressure, intracranial pressure, FVMCA and arterial partial pressure of CO2) during the measurement period are shown in Table 2. A representative example of ABP and FVMCA recordings and the subsequent signal processing from data of a healthy subject and of a patient with severe traumatic brain injury is shown in Fig. 1. Slow blood pressure oscillations in healthy subjects were significantly higher than those in comatose patients [15 mmHg (13/18) vs. 5.3 mmHg (3.9/6.5), p ≤ 0.0001]. However, the height of the amplitudes was not correlated with the status of cerebral autoregulation. In the patients hemispheric difference in ARI was significantly higher than in controls [1.0 (0.3/1.8) vs. 0.5 (0.0/0.5), p ≤ 0.0003]. Therefore data were considered separately for each middle cerebral artery territory. In healthy subjects ARI was 5.0 (5.0/5.5), and the time delay was –2.0 s (–2.7/–1.7). Both autoregulation parameters were significantly lower in patients [ARI 3.3 (2.0/4.5), p ≤ 0.0003; time delay –0.07 s (–0.5/0.45), p ≥ 0.0008]. Figure 2 shows the distribution of ARI and the time delay in healthy and comatose subjects as box and whisker plots.

Representative tracings of raw and processed signals of arterial blood pressure (ABP) and middle cerebral artery flow velocity (FV MCA) from a 29-year-old male healthy subject with an intact cerebral autoregulation (left, A–C) and a 36-year-old male patient recorded on the 9th day of severe traumatic brain injury with impaired cerebral autoregulation (right, D–F). Above Raw data; middle low-pass filtered signals, indicating the slow spontaneous oscillations (healthy B; comatose subject E); below calculated cross-correlation functions with the resulting time delays (healthy C; comatose subject F). Note that with an intact autoregulation slow oscillations of FVMCA (gray line, B) are leading those of ABP (black line, B) as indicated by a time delay of about –1.8 s calculated by the cross-correlation function (C), whereas without autoregulation both signals are almost in line (E), according to a time delay of about –0.2 s (F)

Box and whisker plots illustrate the distribution of autoregulation index (ARI, left) and time delay of cross-correlation analysis (right) in 20 comatose patients (n = 193 measured MCA territories) and 9 healthy subjects (n = 18 measured MCA territories). Line in the box Median; box borders lower and upper quartiles; whiskers minimum and maximum. Data from the comatose subjects include measurements of an impaired and an intact autoregulation, and therefore the results scatter over the whole range. +, x Exceeding values: + > 1.5 box length; x > 3 box length. Significances of median values are given in the text
Intracranial pressure and cerebral perfusion pressure were not correlated with the time delay. Using cerebral perfusion pressure instead of ABP to calculate the time delay for the patients did not affect our statistics and overall results. The correlation between cerebral autoregulation estimated by the cuff deflation test and cross-correlation anal ysis is shown in a scatter diagram (Electronic Supplementary Material, S.F1). Using an ARI of 3.6 and a time delay of –1.06 s as cutoff points (points with maximum κ value) the intermethod agreement in diagnosing an intact or impaired autoregulation was obtained in 108 of 147 recordings (73.5%; Table 3). The κ value (0.44; 95% confidence interval 0.31–0.58) indicated moderate agreement beyond chance.
Discussion
The present study quantified the temporal relationship between spontaneous oscillations of ABP and FVMCA using cross-correlation analysis. In healthy subjects with an intact cerebral autoregulation (as confirmed by the thigh cuff technique), low frequency FVMCA oscillations had a median time delay of about –2.0 s to corresponding ABP oscillations. In contrast, in many analyzed time periods in the patients this phase lead of low frequency FVMCA waves disappeared or became even positive, indicating a disturbance or failure of autoregulation. These results are in accordance with the high pass filter model of cerebral autoregulation [14, 16]. A time delay between slow ABP and FVMCA waves close to 0 s showed that FVMCA passively followed ABP waves, reflecting absence of cerebral autoregulation. In contrast, a negative time delay indicated that FVMCA waves were leading those of ABP, implying an intact (auto)regulatory process. Using this time delay paradigm we were able to distinguish between an impaired and an intact cerebral autoregulation.
Furthermore, with the optimization of our software, for example, by automated exclusion of time periods with insufficient low frequency oscillations, we improved the precision of the technique and also reduced the time required to obtain reliable cross-correlation results compared to earlier studies [18]. In conclusion, we increased the applicability of cross-correlation analysis as a continuous monitor for noninvasive detection of autoregulatory impairment.
Comparison of cross-correlation analysis with the thigh cuff test
The ABP drop induced by the cuff test is not an ideal step decrease but develops within 3–6 s after release of the thigh cuffs [21]. As a result the induced disturbance is in the same (low) frequency range, as the one investigated by cross-correlation analysis. However, our data did not demonstrate a clear correlation between the thigh cuff test and cross-correlation analysis. Nevertheless, intermethod agreement (beyond that expected by chance) in classifying a normal or abnormal cerebral autoregulation was at least moderate (κ = 0.44). Differences between the methods could be explained by the difference in ABP decrease (thigh cuff release 15–30 mmHg, spontaneous oscillations 6–15 mmHg). Furthermore, the thigh cuff test takes the strength of autoregulatory response into account, whereas cross-correlation analysis is based on the temporal characteristics of cerebral autoregulation. In addition, assuming that cerebral autoregulation would be stable over the entire recording time, measurements were done consecutively. According to our own observations and those from others [25], there is considerable short-term variation in cerebral autoregulation as assessed by the ABP/FVMCA relationship, suggesting that this assumption is not fully true. Overall our results suggest that methods seem to be related but it is not justified to use them interchangeably. This is in accordance with the findings of Piechnik et al. [26] who found moderate correlation between the thigh cuff test and the moving correlation coefficient (Mx), a continuous and noninvasive approach similar to the cross-correlation method.
Time delay as a parameter of response latency of cerebral autoregulation
Kuo et al. [27] calculated a time delay of 2.1 s between slow ABP and FVMCA oscillations in a study in 33 healthy volunteers. This is in excellent agreement with our findings and those of several others using different means to investigate the FVMCA response to ABP transients [10, 21, 28]. In a further study Kuo et al. [29] hypothesized that this time delay reflects the response latency of cerebral autoregulation, representing the time that it takes from perception of an ABP change to a response by the resistance vessels. Confirmation of this hypothesis may be supported by results of the Aaslid group [10, 30]. They found that the latency time between sudden changes in ABP and a response of cerebral blood flow and consecutive FVMCA is in the order of 1–2 s. The time for the 50% maximum and peak response is on a scale of 3.5–4 and approx. 7 s, respectively. This suggests that the time delay can serve as a measure of cerebral autoregulatory performance.
Role of intracranial pressure on cerebral autoregulation and the phenomenon of pseudoautoregulation
Using ABP instead of cerebral perfusion pressure to assess cerebral autoregulation in patients with intracranial hypertension may potentially give the wrong impression of intact autoregulation (false or “pseudo”-autoregulation). In this phenomenon a change in ABP directly translates into a parallel change in tissue pressure (i.e., intracranial pressure), not into a “true” response of the resistance vessels. As a result, cerebral blood flow remains constant despite the change in ABP, giving the wrong impression of normal autoregulation when autoregulation assessment is based on measurements of ABP and FVMCA. Since we did not observe a correlation between intracranial pressure and cerebral autoregulation or cerebral perfusion pressure and cerebral autoregulation, we argue that our analysis was not corrupted by the phenomenon of pseudoautoregulation. This is consistent with findings by Lang et al. [31] who applied the moving correlation index to ABP and cerebral perfusion pressure measurements in brain-injured patients. However, we cannot rule out that pseudoautoregulation occurred if our experiments had been conducted at higher levels of intracranial pressure. Czosnyka et al. [32] studied cerebral autoregulation over a wider pressure range in 187 head-injured patients. They reported worsened autoregulation in the presence of very low (< 55 mmHg) or excessive (105 mmHg) cerebral perfusion pressure as well as during intracranial hypertension (intracranial pressure > 25 mmHg), i.e., well above pressures found in our subjects (intracranial pressure 15±6 mmHg and cerebral perfusion pressure 82±12 mmHg). It is unclear how often, where (locally vs. globally), and when pseudoautoregulation occurs [33, 34]. We hypothesize that methods using an ABP challenge to test cerebral autoregulation, such as the thigh cuff test, are particularly prone to detection of pseudoautoregulation, whereas methods using intrinsic ABP fluctuations are less or not at all.
Methodological considerations
Assessing cerebral autoregulation from measurements of ABP and FVMCA is an approximation of complex cerebral hemodynamics. For instance, future work should account for metabolic and neural influences. However, as reflected by the literature, the analysis of spontaneous oscillations between ABP and FVMCA seems to be an accepted model for assessment of cerebral autoregulation. The question of whether relative changes in FVMCA reflect relative changes in flow has been debated previously [10, 28]. The prevailing view is that changes in FVMCA are highly correlated with changes in middle cerebral artery blood flow as long as the middle cerebral artery diameter does not change significantly, which is not the case during analysis over a short period [7, 8, 35]. Moreover, it should be noted that, in comparison to healthy subjects, patients were medicated (analgosedation, vasopressors and osmotic agents) [36, 37] and had different breathing patterns (spontaneous vs. mechanical ventilation) [38, 39, 40]. It is unclear whether either of these factors affected cerebral autoregulation in addition to the injury. This underlines the need of cerebral autoregulation monitoring for assessing the influence of clinical interventions on autoregulatory performance.
Conclusion
The present study demonstrates that cross-correlation analysis may be used to monitor cerebral autoregulation continuously by time delay analysis between slow spontaneous oscillations of ABP and FVMCA. In contrast to short-term autoregulation tests, cross-correlation analysis is simple, noninvasive, and appropriate to measure relative changes in cerebral autoregulation over short periods of time. The time delay of –2.0 s in healthy subjects is in good agreement with other studies and possibly reflects the latency of autoregulatory response. Agreement with the thigh cuff test is rather moderate. Provocation tests of cerebral autoregulation and monitoring techniques based on analysis of slow spontaneous oscillations should not be used interchangeably.
References
Paulson OB, Strandgaard S, Edvinsson L (1990) Cerebral autoregulation. Cerebrovasc Brain Metab Rev 2:161–192
Hlatky R, Furuya Y, Valadka AB, Gonzalez J, Chacko A, Mizutani Y, Contant CF, Robertson CS (2002) Dynamic autoregulatory response after severe head injury. J Neurosurg 97:1054–1061
Lang EW, Diehl RR, Mehdorn HM (2001) Cerebral autoregulation testing after aneurysmal subarachnoid hemorrhage: the phase relationship between arterial blood pressure and cerebral blood flow velocity. Crit Care Med 29:158–163
Robertson CS (2001) Management of cerebral perfusion pressure after traumatic brain injury. Anesthesiology 95:1513–1517
Steiner LA, Czosnyka M, Piechnik SK, Smielewski P, Chatfield D, Menon DK, Pickard JD (2002) Continuous monitoring of cerebrovascular pressure reactivity allows determination of optimal cerebral perfusion pressure in patients with traumatic brain injury. Crit Care Med 30:733–738
Thees C, Scheufler KM, Nadstawek J, Zentner J, Lehnert A, Hoeft A (2003) Monitoring of cerebral perfusion pressure during intracranial hypertension: a sufficient parameter of adequate cerebral perfusion and oxygenation? Intensive Care Med 29:386–390
Newell DW, Aaslid R, Lam A, Mayberg TS, Winn HR (1994) Comparison of flow and velocity during dynamic autoregulation testing in humans. Stroke 25:793–797
Kirkham FJ, Padayachee TS, Parsons S, Seargeant LS, House FR, Gosling RG (1986) Transcranial measurement of blood velocities in the basal cerebral arteries using pulsed Doppler ultrasound: velocity as an index of flow. Ultrasound Med Biol 12:15–21
Tiecks FP, Lam AM, Aaslid R, Newell DW (1995) Comparison of static and dynamic cerebral autoregulation measurements. Stroke 26:1014–1019
Aaslid R, Lindegaard KF, Sorteberg W, Nornes H (1989) Cerebral autoregulation dynamics in humans. Stroke 20:45–52
Giller CA (1991) A bedside test for cerebral autoregulation using transcranial Doppler ultrasound. Acta Neurochir (Wien) 108:7–14
Tiecks FP, Douville C, Byrd S, Lam AM, Newell DW (1996) Evaluation of impaired cerebral autoregulation by the Valsalva maneuver. Stroke 27:1177–1182
Reinhard M, Muller T, Guschlbauer B, Timmer J, Hetzel A (2003) Transfer function analysis for clinical evaluation of dynamic cerebral autoregulation-a comparison between spontaneous and respiratory-induced oscillations. Physiol Meas 24:27–43
Zhang R, Zuckerman JH, Giller CA, Levine BD (1998) Transfer function analysis of dynamic cerebral autoregulation in humans. Am J Physiol 274:H233–H241
Giller CA (1990) The frequency-dependent behavior of cerebral autoregulation. Neurosurgery 27:362–368
Diehl RR, Linden D, Lucke D, Berlit P (1998) Spontaneous blood pressure oscillations and cerebral autoregulation. Clin Auton Res 8:7–12
Steinmeier R, Bauhuf C, Hubner U, Bauer RD, Fahlbusch R, Laumer R, Bondar I (1996) Slow rhythmic oscillations of blood pressure, intracranial pressure, microcirculation, and cerebral oxygenation. Dynamic interrelation and time course in humans. Stroke 27:2236–2243
Steinmeier R, Hofmann RP, Bauhuf C, Hubner U, Fahlbusch R (2002) Continuous cerebral autoregulation monitoring by cross-correlation analysis. J Neurotrauma 19:1127–1138
Christ M, Hagmueller A, Morgenstern U, Theilen H, Ragaller M, Steinmeier R (2004) Continuous and non-invasive assessment of cerebral autoregulation by cross-correlation analysis. Intensive Care Med S169:651
Mascia L, Fedorko L, terBrugge K, Filippini C, Pizzio M, Ranieri VM, Wallace MC (2003) The accuracy of transcranial Doppler to detect vasospasm in patients with aneurysmal subarachnoid hemorrhage. Intensive Care Med 29:1088–1094
Mahony PJ, Panerai RB, Deverson ST, Hayes PD, Evans DH (2000) Assessment of the thigh cuff technique for measurement of dynamic cerebral autoregulation. Stroke 31:476–480
Lang EW, Diehl RR, Timmermann L, Baron R, Deuschl G, Mehdorn HM, Zunker P (1999) Spontaneous oscillations of arterial blood pressure, cerebral and peripheral blood flow in healthy and comatose subjects. Neurol Res 21:665–669
Kuusela TA, Kaila TJ, Kahonen M (2003) Fine structure of the low-frequency spectra of heart rate and blood pressure. BMC Physiol 3:11
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174
Panerai RB, Carey BJ, Potter JF (2003) Short-term variability of cerebral blood flow velocity responses to arterial blood pressure transients. Ultrasound Med Biol 29:31–38
Piechnik SK, Yang X, Czosnyka M, Smielewski P, Fletcher SH, Jones AL, Pickard JD (1999) The continuous assessment of cerebrovascular reactivity: a validation of the method in healthy volunteers. Anesth Analg 89:944–949
Kuo TB, Chern CM, Sheng WY, Wong WJ, Hu HH (1998) Frequency domain analysis of cerebral blood flow velocity and its correlation with arterial blood pressure. J Cereb Blood Flow Metab 18:311–318
Panerai RB, Dawson SL, Eames PJ, Potter JF (2001) Cerebral blood flow velocity response to induced and spontaneous sudden changes in arterial blood pressure. Am J Physiol Heart Circ Physiol 280:H2162–H2174
Kuo TB, Chern CM, Yang CC, Hsu HY, Wong WJ, Sheng WY, Hu HH (2003) Mechanisms underlying phase lag between systemic arterial blood pressure and cerebral blood flow velocity. Cerebrovasc Dis 16:402–409
Aaslid R, Newell DW, Stooss R, Sorteberg W, Lindegaard KF (1991) Assessment of cerebral autoregulation dynamics from simultaneous arterial and venous transcranial Doppler recordings in humans. Stroke 22:1148–1154
Lang EW, Lagopoulos J, Griffith J, Yip K, Mudaliar Y, Mehdorn HM, Dorsch NW (2003) Noninvasive cerebrovascular autoregulation assessment in traumatic brain injury: validation and utility. J Neurotrauma 20:69–75
Czosnyka M, Smielewski P, Piechnik S, Steiner LA, Pickard JD (2001) Cerebral autoregulation following head injury. J Neurosurg 95:756–763
Enevoldsen EM, Jensen FT (1977) “False” autoregulation of cerebral blood flow in patients with acute severe head injury. Acta Neurol Scand Suppl 64:514–515
Sahuquillo J, Amoros S, Santos A, Poca MA, Valenzuela H, Baguena M, Garnacho A (2000) False autoregulation (pseudoautoregulation) in patients with severe head injury. Its importance in CPP management. Acta Neurochir (Wien) Suppl 76:485–490
Serrador JM, Picot PA, Rutt BK, Shoemaker JK, Bondar RL (2000) MRI measures of middle cerebral artery diameter in conscious humans during simulated orthostasis. Stroke 31:1672–1678
Myburgh JA, Upton RN, Grant C, Martinez A (2003) The effect of infusions of adrenaline, noradrenaline and dopamine on cerebral autoregulation under propofol anaesthesia in an ovine model. Intensive Care Med 29:817–824
Johnston AJ, Steiner LA, O'Connell M, Chatfield DA, Gupta AK, Menon DK (2004) Pharmacokinetics and pharmacodynamics of dopamine and norepinephrine in critically ill head-injured patients. Intensive Care Med 30:45–50
Eames PJ, Panerai RB, Potter JF (2004) Influence of controlled breathing patterns on cerebrovascular autoregulation and cardiac baroreceptor sensitivity. Clin Sci (Lond) 106:155–162
Zwiener U, Walter B, Kratzsch B, Bauer R (2003) Marked reduction of brainstem blood flow in artificially ventilated newborn piglets during normoxia and normocapnic hypoxia. Intensive Care Med 29:2277–2284
Mascia L, Grasso S, Fiore T, Bruno F, Berardino M, Ducati A (2005) Cerebro-pulmonary interactions during the application of low levels of positive end-expiratory pressure. Intensive Care Med 31:373–379
Acknowledgements
We sincerely thank G. Elmer and S. Stöhrer for their help in data acquisition.
Author information
Authors and Affiliations
Corresponding author
Additional information
Financial support for this study was provided by Kuratorium ZNS, Hannelore Kohl Stiftung, Bonn, Germany (no. 2001011).
Electronic supplementary material
Rights and permissions
About this article
Cite this article
Christ, M., Noack, F., Schroeder, T. et al. Continuous cerebral autoregulation monitoring by improved cross-correlation analysis: comparison with the cuff deflation test. Intensive Care Med 33, 246–254 (2007). https://doi.org/10.1007/s00134-006-0451-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-006-0451-8