
Summary
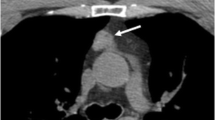
Surgical or conservative treatment of ACTH-producing tumors results in acute drop of the previously excessively high cortisol levels. The following associated pathophysiological changes also occur in the organism's recovery from stress, such as trauma, operation or chemotherapy of tumors. Both cases result in a regeneration of the immune system, which might even be exalted. The corresponding radiographic feature is the ”rebound” enlargement of the thymus occuring about six months after remission of hypercortisolism. Histological examination reveals benign thymus hyperplasia. Especially in cases of still unkown primary tumor the appereance of this anterior mediastinal mass can lead to misdiagnosis. We present the cases of two patients with diffuse thymic hyperplasia following surgical and medical correction of hypercortisolism. One patient suffered from classic Cushing's disease responding to transsphenoidal resection of an ACTH-secreting pituitary microadenoma. Six months later CT of the chest incidentally demonstrated an anterior mediastinal mass known as thymic hyperplasia. The second patient presented with an ectopic, still unkown source of ACTH-production. Six months after medical correction of hypercortisolism CT of the thorax showed an enlargement of the anterior mediastinum. Thymectomy was performed in order to exclude thymus carcinoid. Histological examination revealed benign thymus hyperplasia with negative immunostaining.
Conclusion: Radiologists and clinicians should be familiar with the pathophysiological changes resulting from precipitously dropping cortisol levels in order to prevent diagnostic errors and unnecessary operations.
Zusammenfassung
Durch operative oder medikamentöse Therapie von ACTH-produzierenden Tumoren wird der exzessiv erhöhte Kortisolspiegel abrupt korrigiert. Die damit verbundenen pathopysiologischen Veränderungen entsprechen der Erholungsphase des Organismus nach extremer Streßbelastung durch Trauma, Operation oder Chemotherapie von Tumoren. In beiden Fällen kommt es zu einer – möglicherweise sogar überschießenden – Regeneration des Immunsystems. In der bildgebenden Diagnostik ist dies als „Rebound“thymushyperplasie zu beobachten. Diese ca. 6 Monate posttherapeutisch auftretende anteriore mediastinale Raumforderung kann besonders in Fällen von noch unbekanntem Primärtumor zu Fehldiagnosen Anlaß geben. Anhand der beiden folgenden Kasuistiken wird versucht, den pathophysiologischen und zeitlichen Zusammenhang zwischen dem Kortisolabfall und der reaktiven Thymusvergrößerung dem Diagnostiker und dem Therapeuten ins Bewußtsein zu rufen.
Similar content being viewed by others


Author information
Authors and Affiliations
Additional information
Eingegangen am 26. Mai 1997 Angenommen am 26. August 1997
Rights and permissions
About this article
Cite this article
Schmidt, S., Klose, K., Frank, M. et al. Reactive thymic hyperplasia following treatment of ACTH-producing tumors. Radiologe 37, 913–917 (1997). https://doi.org/10.1007/s001170050302
Issue Date:
DOI: https://doi.org/10.1007/s001170050302