
Abstract
Background
Many studies have established intravenous corticosteroid as an effective prophylactic therapy in fat embolism syndrome (FES). However, its use is limited among surgeons because of systemic side effects. Inhalational steroids have least systemic effects and are widely used for several chest conditions (i.e., asthma), but their effectiveness in FES has not been established.
Question/purpose
This study was sought to evaluate the (1) efficacy and (2) safety of inhalational Ciclesonide (CIC) in prevention of FES and treatment of hypoxemia in isolated skeletal trauma victims.
Methods
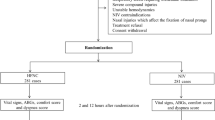
A nonrandomized prospective control trial was designed in which all patients between 18 and 40 years with isolated skeletal injury who presented within 8 h of injury were allocated to either Trial group or control group. Trial group patients received 640 mcg of inhalational CIC with a metered-dose inhaler at the time of admission, and at 24 h. Control group patients did not receive any prophylactic therapy. Both groups were evaluated for development of FES (Gurd’s criteria) and hypoxemia (PaO2 <70 mmHg) for 72 h. The complications related to CIC administration were evaluated in trial group patients during their hospital stay.
Results
Of 35 patients in each group, two patients in Trial group and nine patients in control group developed FES (P = 0.022). Eight patients in Trial group had hypoxemia at the time of admission, six of them improved and one additional patient developed hypoxemia after inhalational CIC administration. In control group, ten patients had hypoxia at the time of admission, only one of them improved and remaining nine patients had persistent hypoxemia even after 72 h. Additionally, three patients developed hypoxemia. A significant improvement in hypoxemia and a significant decrease in the incidence of FES were observed in Trial group (P < 0.05) compared to control group. None of the patients presented with any complications or adverse effects of steroid in Trial group.
Conclusion
Inhalational CIC is a safe and effective therapy for prevention of FES and also an effective drug for treatment of hypoxemia in orthopedic trauma victims.
Level of evidence
Level III, therapeutic study.

Similar content being viewed by others

References
Levy D. The fat embolism syndrome. Clin Orthop. 1990;261:262–91.
Sen RK, Tripathy SK, Krishnan V. Role of corticosteroid as a prophylactic measure in fat embolism syndrome: a literature review. Musculoskelet Surg. 2012;96(1):1–8.
Sproule BJ, Brady JL, Gilbert J. Studies on the syndrome of fat embolization. Canad Med Ass J. 1964;90:1244–7.
Wertzberger JL, Peltier LF. Fat embolism: the importance of arterial hypoxia. Surg Annu. 1968;63:626–9.
Duis HJ. The fat embolism syndrome. Injury. 1997;28(2):77–85.
Filomeno ITB, Carelli CR, Amatuzzi MM. Fat embolism: a review for current orthopedics practice. Acta Orthop Bras. 2005;13(4):1–34.
Gupta B, D’souza N, Sawhney C, Farooque K, Kumar A, Agrawal P, Misra MC. Analyzing fat embolism syndrome in trauma patients at AIIMS Apex Trauma Center, New Delhi, India. J Emerg Trauma Shock. 2011;4:337–41.
Jain S, Mittal M, Kansal A, Singh Y, Kolar PR, Jain S. Fat embolism syndrome. J Assoc Physician India. 2008;56:245–9.
Gunther H. New developments in corticosteroids. Proc Am Thorac Soc. 2004;1:269–74.
Kallenbach J, Lewis M, Zaltzman M, Feldman C, Orford A, Zwi S. ‘Low-dose’ corticosteroid prophylaxis against fat embolism. J Trauma. 1987;27:1173–6.
Lindeque BG, Schoeman HS, Dommisse GF, Boeyens MC, Vlok AL. Fat embolism and the fat embolism syndrome: a double-blind therapeutic study. J Bone Joint Surg Br. 1987;69:128–31.
Stoltenberg JJ, Gustilo RB. The use of methylprednisolone and hypertonic glucose in the prophylaxis of fat embolism syndrome. Clin Orthop Relat Res. 1979;143:211–21.
Nave R, Zech K, Bethke TD. Lower oropharyngeal deposition of inhaled ciclesonide via hydrofluoroalkane metered-dose inhaler compared with budesonide via chlorofluorocarbon metered-dose inhaler in healthy subjects. Eur J Clin Pharmacol. 2005;61:203–8 (nu 1968; 63: 626-9).
Richter K, Kanniess F, Biberger C, Nave R, Magnussen H. Comparison of the oropharyngeal deposition of inhaled Ciclesonide and fluticasone propionate in patients with asthma. J Clin Pharmacol. 2005;45:146–52.
Schaffner TJ, Skoner DP. Ciclesonide: a safe and effective inhaled corticosteroid for the treatment of asthma. J Asthma Allergy. 2009;2:25–32.
Mouloudi E, Georgopoulos D. Treatment with aerosols in mechanically ventilated patients: is it worthwhile? Curr Opin Anaesthesiol. 2002;15:103–9.
Agarwal A, Sen R, Tripathy SK, et al. Is there any role of inhalational corticosteroids in the prophylaxis of post-traumatic fat embolism syndrome? Cureus. 2015;7(9):e332. doi:10.7759/cureus.332.
Gurd AR. Fat embolism: an aid to diagnosis. J Bone Joint Surg(Br). 1970;52:732–77.
Schonfeld SA, Ploysongsang Y, DiLisio R, et al. Fat embolism prophylaxis with corticosteroids. Ann Int Med. 1983;99:438–43.
Szefler S, Rohatagi S, Williams J, Lloyd M, Kundu S, Banerji D. Ciclesonide, a novel inhaled steroid, does not affect hypthalamic-pituitaryadrenal axis function in patients with moderate-to-severe persistent asthma. Chest. 2005;128:1104–14.
Wang J, Winskog C, Edston E, Walther SM. Inhaled and intravenous corticosteroids both attenuate chlorine gas-induced lung injury in pigs. J Trauma. 2000;48:562–72.
Melanie H, Gunther H, Hartmut R. Comparative pharmacology, bioavaibility, pharmacokinetics, pharmacodynamics of inhaled glucocorticosteroids. Immunol Allergy Clin N Am. 2005;25:469–88.
Prakash S, Sen RK, Tripathy SK, Sen IM, Sharma RR, Sharma S. Role of Interleukin-6 as an early marker of fat embolism syndrome: a clinical study. Clin Orthop Relat Res. 2013 Feb 20. (Epub ahead of print).
Lapinsky SE, Granton JT. Respiratory system: critical care lessons from severe acute respiratory syndrome. Curr Opin Crit Care. 2004;10:53–8.
Lipworth BJ, Kaliner MA, LaForce CF, Baker JW, Kaiser HB, Amin D, et al. Effect of ciclesonide and fluticasone on hypothalamic-pituitary-adrenal axis function in adults with mild-to-moderate persistent asthma. Ann Allergy Asthma Immunol. 2005;94:465–72.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The institutional ethics Committee permission was obtained before initiating the study.
Conflict of interest
Ramesh Kumar Sen, Shiva Prakash, Sujit Kumar Tripathy, Amit Agrawal and Indu Mohini Sen declare that they have no conflict of interest.
Source of support/funding
This project was supported by the AADO Research Fund.
Rights and permissions
About this article

Cite this article
Sen, R.K., Prakash, S., Tripathy, S.K. et al. Inhalational Ciclesonide found beneficial in prevention of fat embolism syndrome and improvement of hypoxia in isolated skeletal trauma victims. Eur J Trauma Emerg Surg 43, 313–318 (2017). https://doi.org/10.1007/s00068-016-0633-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-016-0633-1