
Abstract
Purpose
To evaluate the feasibility of hypofractionation with SIB in all settings in Germany to prepare a multicenter treatment comparison.
Methods
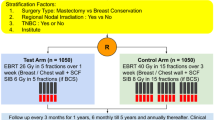
Eligible patients had histopathologically confirmed breast cancer operated by BCS. Patients received WBI 40.0 Gy in 16 fractions of 2.5 Gy. A SIB with 0.5 Gy per fraction was administered to the tumor bed, thereby giving 48.0 Gy in 16 fractions to the boost-PTV sparing heart, LAD, lung, contralateral breast. The primary study objective was feasibility, administration of specified dose in 16 fractions within 22–29 days with adherence to certain dose constraints (heart; LAD; contralateral breast); secondary endpoints were toxicity, QoL.
Results
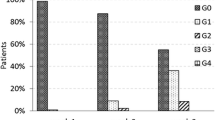
151 patients were recruited from 7 institutions between 07/11-10/12. 10 patients met exclusion criteria prior to irradiation. All but two patients (99 %) received the prescribed dose in the PTVs. Adherence to dose constraints and time limits was achieved in 89 % (95 % CI 82 % to 93 %). 11 AE were reported in 10 patients; five related to concurrent endocrine therapy. Two of the AEs were related to radiotherapy: grade 3 hot flushes in two cases. QoL remained unchanged.
Conclusion
Hypofractionation with a SIB is feasible and was well tolerated in this study.
Zusammenfassung
Hintergrund
Die ARO-2010-01-Studie prüfte die Durchführbarkeit einer hypofraktionierten Bestrahlung mit simultan-integriertem Boost (SIB) in unterschiedlichen Versorgungseinrichtungen zur Vorbereitung einer multizentrischen Vergleichsstudie.
Methoden
In die Studie rekrutiert wurden Patientinnen mit histopathologisch gesichertem Mammakarzinom nach brusterhaltender Operation. Bestrahlt wurde die Brust mit 40,0 Gy in 16 Fraktionen à 2,5 Gy Einzeldosis; zusätzlich wurde bei jeder Fraktion ein simultan- integrierter Boost mit 0,5 Gy appliziert, so dass im Boost-PTV (Planungszielvolumen) eine Dosis von 48 Gy in 16 Fraktionen erreicht wurde. Das primäre Zielkriterium war die Durchführbarkeit, definiert als Verabreichung von 48 Gy GD in 16 Fraktionen in mindestens 22 d bis maximal 29 d Therapiezeit unter Einhaltung von Grenzdosen (Lunge, Herz, LAD, kontralaterale Brust); sekundäre Endpunkte waren Toxizität und Lebensqualität.
Ergebnisse
Zwischen 07/2011 und 10/2012 wurden 151 Patientinnen in 7 Prüfzentren rekrutiert. Bei 10 Patientinnen wurden vor der Strahlentherapie Ausschlusskriterien festgestellt. Fast alle Patientinnen (99 %) erhielten die verschriebene Dosis im PTV. Grenzdosen und Zeitlimits wurden in 89 % (95 % CI 82 % bis 93 %) eingehalten. 11 unerwünschte Ereignisse wurden bei 10 Patientinnen gemeldet; fünf in Verbindung mit gleichzeitiger endokriner Therapie. In 2 Fällen wurde eine kausale Beziehung zur Strahlentherapie angegeben: Grad-3-Hitzewallungen. Die Lebensqualität blieb unverändert.
Schlussfolgerungen
Die hypofraktionierte Bestrahlung mit simultan-integriertem Boost konnte in dieser multizentrischen Studie in Praxen und Strahlenkliniken problemlos durchgeführt werden. Die Verträglichkeit war in dieser Studie gut.




Similar content being viewed by others

Abbreviations
- 3D-CRT:
-
Three-dimensional conformal radiotherapy
- AE:
-
Adverse event
- ARO:
-
Arbeitsgemeinschaft Radiologische Onkologie (Research Group on Radiological Oncology in the German Cancer Society)
- BCS:
-
Breast-conserving surgery
- CR:
-
Conventional radiotherapy
- DLco:
-
Diffusing capacity of the lung for carbon monoxide
- DVH:
-
Dose–volume histogram
- EORTC:
-
European Organisation for Research and Treatment of Cancer
- FEV1:
-
Forced expiratory volume in 1 s
- IMRT:
-
Intensity modulated radiotherapy
- LAD:
-
Left coronary artery
- NCI-CTC:
-
National Cancer Institute Common Toxicity Criteria
- PTV:
-
Planning target volume
- RIVA:
-
Ramus interventriculares anterior
- SIB:
-
Simultaneous integrated boost
- TT:
-
Tomotherapy
- VMAT:
-
Volumetric modulated arc therapy
- WBI:
-
Whole breast irradiation
References
Clarke M, Collins R, Darby S et al, Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) (2005) Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet 366:2087–2106
Darby S, McGale P, Correa C et al (2011) Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet 378:1707–1716
Whelan TJ, Julian J, Wright J et al (2000) Does locoregional RT improve survival in breast cancer? A meta-analysis. J Clin Oncol 18:1220–1229
Bartelink H, Horiot JC, Poortmans P et al (2007) Impact of a higher radiation dose on local control and survival in breast-conserving therapy of early breast cancer: 10-year results of the randomized boost versus no boost EORTC 22881-10882 trial. J Clin Oncol 22:3259–3326
Livi L, Borghesi S, Saieva C et al (2009) Benefit of radiation boost after whole-breast radiotherapy. Int J Radiat Oncol Biol Phys 75:1029–1034
Azria D, Auvray H, Barillot I et al (2008) Ductal carcinoma in situ: role of the boost. Cancer Radiother 12:571–576
Whelan TJ, Pignol JP, Levine MN et al (2010) Long-term results of hypofractionated radiation therapy for breast cancer. N Engl J Med 362:513–520
START Trialists’ Group, Bentzen SM, Agrawal RK, Aird EG et al (2008) The UK Standardization of Breast Radiotherapy (START) Trial A of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial. Lancet Oncol 9:331–341
START Trialists’ Group, Bentzen SM, Agrawal RK, Aird EG et al (2008) The UK Standardization of Breast Radiotherapy (START) Trial B of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial. Lancet 371:1098–1107
Owen JR, Ashton A, Bliss JM et al (2006) Effect of radiotherapy fraction size on tumour control in patients with early-stage breast cancer after local tumour excision: long-term results of a randomized trial. Lancet Oncol 7:467–471
Sedlmayer F, Sautter-Bihl ML, Budach W et al (2013) Breast Cancer Expert Panel of the German Society of Radiation Oncology (DEGRO). Is the simultaneously integrated boost (SIB) technique for early breast cancer ready to be adopted for routine adjuvant radiotherapy? Statement of the German and the Austrian Societies of Radiooncology (DEGRO/ÖGRO). Strahlenther Onkol 189:193–196
Sedlmayer F, Sautter-Bihl ML, Budach W et al (2013) Breast Cancer Expert Panel of the German Society of Radiation Oncology (DEGRO). DEGRO practical guidelines: radiotherapy of breast cancer I. Radiotherapy following breast conserving therapy for invasive breast cancer. Strahlenther Onkol 189:825–833
Chadha M, Vongtama D, Friedmann P et al (2012) Comparative acute toxicity from whole breast irradiation using 3-week accelerated schedule with concomitant boost and the 6.5-week conventional schedule with sequential boost for early-stage breast cancer. Clin Breast Cancer 12:57–62
Van Parijs HM, Vinh-Hung V et al (2012) Short course radiotherapy with simultaneous integrated boost for stage I–II breast cancer, early toxicities of a randomized clinical trial. Radiat Oncol 7:80
Scorsetti M, Alongi F, Fogliata A et al (2012) Phase I–II study of hypofractionated simultaneous integrated boost using volumetric modulated arc therapy for adjuvant radiation therapy in breast cancer patients: a report of feasibility and early toxicity results in the first 50 treatments. Radiat Oncol 28:145
Darby SC, Ewertz M, McGale P et al (2012) Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med 368:987–998
Compliance with ethical guidelines
Conflict of interest
K. Dellas, R. Vonthein, J. Zimmer, S. Dinges, A.D. Boivcev, P. Andreas, D. Fischer, C. Winkler, A. Ziegler, and J. Dunst state that there are no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
ARO Study Group
Rights and permissions
About this article

Cite this article
Dellas, K., Vonthein, R., Zimmer, J. et al. Hypofractionation with simultaneous integrated boost for early breast cancer. Strahlenther Onkol 190, 646–653 (2014). https://doi.org/10.1007/s00066-014-0658-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-014-0658-5