
Abstract
Purpose:
The purpose of this study was to analyze the probability and time course of fibrotic changes in breast reconstruction before or after postmastectomy radiotherapy (PMRT).
Materials and Methods:
Between 1995 and 2004, 109 patients were treated with PMRT at Tübingen University and underwent heterologous (HL) or autologous (AL) breast reconstruction prior or subsequent to radiation therapy. Fibrosis of the reconstructed breast after radiotherapy was assessed using the Baker score for HL reconstructions and the Common Terminology Criteria for Adverse Events (CTCAE) for all patients. Actuarial rates of fibrosis were calculated for the maximum degree acquired during follow- up and at the last follow-up visit documented.
Results:
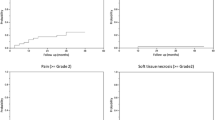
Median time to follow-up was 34 months (3–227 months). Radiotherapy was applied with a median total dose of 50.4 Gy. A total of 44 patients (40.4%) received a boost treatment with a median dose of 10 Gy. Breast reconstruction was performed with AL, HL, or combined techniques in 20, 82, and 7 patients, respectively. The 3-year incidence of ¡Ý grade III maximum fibrosis was 20% and 43% for Baker and CTCAE scores, respectively. The corresponding figures for fibrosis at last follow-up visit were 18% and 2%. The 3-year rate of surgical correction of the contralateral breast was 30%. Initially unplanned surgery of the reconstructed breast was performed in 39 patients (35.8%). Boost treatment and type of cosmetic surgery (HL vs. AL) were not significantly associated with the incidence of fibrosis.
Conclusions:
We found severe fibrosis to be a frequent complication after PMRT radiotherapy and breast reconstruction. However, surgical intervention can ameliorate the majority of high grade fibrotic events leading to acceptable long-term results. No treatment parameters associated with the rate of fibrosis could be identified.
Zusammenfassung
Zielsetzung:
Ziel der Arbeit war es, die Frequenz und den zeitlichen Verlauf fibrotischer Veränderungen nach Thoraxwandbestrahlung und plastischer Rekonstruktion der Mamma zu analysieren.
Material und Methoden:
Zwischen 1995 und 2004 wurde bei 109 Patientinnen in der Klinik für Radioonkologie des Universitätsklinikums Tübingen eine Thoraxwandbestrahlung nach Mastektomie durchgeführt. Vor oder nach der Bestrahlung erfolgte eine autologe (AL) oder heterologe (HL) Brustrekonstruktion. Fibrotische Veränderungen der rekonstruierten Brust wurden retrospektiv anhand des Baker-Scores (AL) bzw. der Definition der Common Terminology Criteria for Adverse Events (CTCAE) erhoben. Es wurden aktuarische Raten der stärksten beobachteten Ausprägung der Fibrose bzw. des Fibrosegrades zum letzten Beobachtungszeitpunkt für beide Scores erhoben.
Ergebnisse:
Die mediane Nachbeobachtungszeit betrug 34 Monate (3–227). Die Strahlentherapie wurde mit einer medianen Gesamtdosis von 50.4 Gy appliziert. 44 Patientinnen (40.4%) erhielten eine Boostbestrahlung mit einer medianen Gesamtdosis von 10 Gy. Die Brustrekonstruktion erfolgte in AL- bzw. HL- oder kombinierter Technik bei 20, 82, bzw. 7 Patientinnen. Die 3-Jahresinzidenz der maximal beobachteten Fibrose ¡Ý Grad III betrug 20% nach der Baker-Klassifikation bzw. 43% nach CTCAE-Score. Die entsprechenden Fibroseraten für den letzten Beobachtungszeitpunkt betrugen 18% bzw. 2%. Die 3-Jahresrate operativer Korrekturen der kontralateralen Brust betrug 30%. Bei 39 Patientinnen (35.8 %) wurden initial ungeplante operative Zweiteingriffe an der rekonstruierten Brust durchgeführt. Die Boostbestrahlung und die Rekonstruktionstechnik (AL bzw. HL) hatten keinen signifikanten Einfluss auf die Fibroserate.
Schlussfolgerung:
Höhergradige Fibrosen stellen eine regelmäßige Komplikation nach Thoraxwandbestrahlung und plastischer Brustrekonstruktion dar. Offenbar kann der überwiegende Teil der fibrotischen Komplikationen operativ korrigiert werden. Wir konnten keine Risikofaktoren für die Entwicklung höhergradiger Fibrosen identifizieren.
Similar content being viewed by others


References
Azria D, Gourgou S, Sozzi WJ, et al. Concomitant use of tamoxifen with radiotherapy enhances subcutaneous breast fibrosis in hypersensitive patients. Br J Cancer 2004;91:1251–60
Bentzen SM, Skoczylas JZ, Overgaard M, Overgaard J. Radiotherapy-related lung fibrosis enhanced by tamoxifen. J Natl Cancer Inst 1996;88:918–22
Chang DW, Barnea Y, Robb GL. Effects of an autologous flap combined with an implant for breast reconstruction: An evaluation of 1000 consecutive reconstructions of previously irradiated breasts. Plast Reconstr Surg 2008;122:356–62
Chawla AK, Kachnic LA, Taghian AG, et al. Radiotherapy and breast reconstruction: complications and cosmesis with TRAM versus tissue expander/ implant. Int J Radiat Oncol Biol Phys 2002;54:520–6
Contant CM, van Geel AN, van der Holt B, et al. Morbidity of immediate breast reconstruction (IBR) after mastectomy by a subpectorally placed silicone prosthesis: the adverse effect of radiotherapy. Eur J Surg Oncol 2000;26:344–50
Cordeiro PG, Pusic AL, Disa JJ, et al. Irradiation after immediate tissue expander/implant breast reconstruction: Outcomes, complications, aesthetic results, and satisfaction among 156 patients. Plast Reconstr Surgery 2004;113:877–81
Early Breast Cancer Trialists’ Collaborative Group. Favourable and unfavourable effects on long-term survival of radiotherapy for early breast cancer: an overview of the randomised trials. Lancet 2000;355:1757–70
Hammer J, Track C, Seewald DH, et al. Local relapse after breast-conserving surgery and radiotherapy: effects on survival parameters. Strahlenther Onkol 2009;185:431–7
Hoeller U, Borgmann K, Feyer P, Souchon R. On the interactions of adjuvant radiotherapy and tamoxifen treatment for breast cancer. Strahlenther Onkol 2007;183:535–44
Hoeller U, Grzyska B, Lorenzen J, et al. Is grading of breast fibrosis with mammography feasible? Strahlenther Onkol 2005;181:307–12
Jhaveri JD, Rush SC, Kostroff K, et al. Clinical outcomes of postmastectomy radiation therapy after immediate breast reconstruction. Int J Rad Oncol Biol Phys 2008;72:859–65
Kreienberg R, Kopp I, Albert U, et al. Interdisciplinary S3-guidelines for diagnosis, treatment and follow-up of breast cancer. Zuckschwerdt, Germering bei München: 2008
Kronowitz SJ, Robb GL, Radiation therapy and breast reconstruction: a critical review of the literature. Plast Recostr Surg 2009;124:395–408
Krueger EA, Wilkins EG, Strawderman M, et al. Complications and patient satisfaction following expander/implantat breast reconstruction with and without radiotherapy. Int J Radiat Oncol Biol Phys 2001;49:713–21
Kuske RR, Schuster R, Klein E, et al. Radiotherapy and breast reconstruction: clinical results and dosimetry. Int J Radiat Oncol Biol Phys 1991;21: 339–46
Little G, Baker JL. Results of closed compression capsulotomy for treatment of contracted breast implant capsules. Plast Reconstr Surg 1980;65: 30–3
Piroth MD, Piroth DM, Pinkawa M, et al. Immediate reconstruction with an expander/implant following ablatio mammae because of breast cancer: side effects and cosmetic results after adjuvant chest wall radiotherapy. Strahlenther Onkol 2009;185:669–74
Poortmans PM, Collette L, Horiot JC, et al. Impact of the boost dose of 10 Gy versus 26 Gy in patients with early stage breast cancer after a microscopically incomplete lumpectomy: 10-year results of the randomised EORTC boost trial. Radiother Oncol 2009;90:80–5
Rowell NP. Radiotherapy to the chest wall following mastectomy for nodenegative breast cancer: a systematic review. Radiother Oncol 2009;91: 23–32
Sauer R, Schulz KD, Hellriegel KP. Strahlentherapie nach Mastektomie – Interdisziplinärer Konsensus beendet Kontroverse. Strahlenther Onkol 2001;177:1–9
Spear SL, Newman MK, Bedford MS, et al. A Retrospective analysis of outcomes using three common methods for immediate breast reconstruction. Plast Reconstr Surg 2008;122:340–7
Tran NV, Chang DW, Gupta A, et al. Comparison of immediate and delayed free TRAM flap breast reconstruction in patients receiving postmastectomy radiation therapy. Plast Reconstr Surg 2001;108:78–82
Van de Steene J, Soete G, Storme G. Adjuvant radiotherapy for breast cancer significantly improves overall survival: the missing link. Radiother Oncol 2000;55:263–72
Victor SJ, Brown DM, Horwitz EM, et al. Treatment outcome with radiation therapy after breast augmentation or reconstruction in patients with primary breast carcinoma. Cancer 1998;82:1303–9
Vinh-Hung V, Truong PT, Janni W, et al. The effect of adjuvant radiotherapy on mortality differs according to primary tumor location in women with node-positive breast cancer. Strahlenther Onkol 2009;185:161–8
Voordeckers M, Vinh-Hung V, Lamote J, et al. Survival benefit with radiation therapy in node-positive breast carcinoma patients. Strahlenther Onkol 2009;185:656–62
Whelan TJ, Julian J, Wright J, et al. Does locoregional radiation therapy improve survival in breast cancer? A meta-analysis. J Clin Oncol 2000;18: 1220–9
Whitfield GA, Horan G, Irwin MS, et al. Incidence of severe capsular contracture following implant-based immediate breast reconstruction with or without postoperative chest wall radiotherapy using 40 Gray in 15 fractions. Radiother Oncol 2009;90:141–7
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Claßen, J., Nitzsche, S., Wallwiener, D. et al. Fibrotic Changes after Postmastectomy Radiotherapy and Reconstructive Surgery in Breast Cancer. Strahlenther Onkol 186, 630–636 (2010). https://doi.org/10.1007/s00066-010-2158-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-010-2158-6