
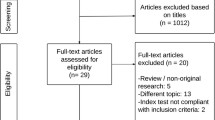
Abstract
Background
Dietary restriction together with alteration of the gastrointestinal tract results in major metabolic changes and significant weight loss in patients undergoing bariatric surgery. Current methods of measuring these changes are often inaccurate and lack a molecular basis. The objective of this study was to determine the role of exhaled ketones as non-invasive markers of nutritional status in patients undergoing surgical treatment of obesity.
Methods
Patients at different stages of treatment for obesity were recruited to this single-centre cross-sectional study. The sample time points were as follows: (i) at the time of initial attendance prior to dietary or surgical interventions, (ii) on the day of surgery following a low carbohydrate diet, and (iii) > 3 months after either Roux-en-Y gastric bypass or sleeve gastrectomy. The concentrations of ketones within breath samples were analysed by selected ion flow tube mass spectrometry.
Results
Forty patients were recruited into each of the three study groups. Exhaled acetone concentrations increased significantly following pre-operative diet (1396 ppb) and bariatric surgery (1693 ppb) compared to the start of treatment (410 ppb, P < 0.0001). In comparison, concentrations of heptanone (6.5 vs. 4.1 vs. 1.4 ppb, P = 0.021) and octanone (3.0 vs. 1.4 vs. 0.7 ppb, P = 0.021) decreased significantly after dieting and surgical intervention. Exhaled acetone (ρ − 0.264, P = 0.005) and octanone (ρ 0.215, P = 0.022) concentrations were observed to correlate with excess body weight at the time of sampling. Acetone and octanone also correlated with neutrophil and triglyceride levels (P < 0.05).
Conclusion
Findings confirm breath ketones, particularly acetone, to be a potentially clinically useful method of non-invasive nutritional assessment in obese patients.
Similar content being viewed by others
Background
Obesity (body mass index (BMI), > 30 kg/m2) is a global health epidemic with over 600 million adults, > 10% of the world’s population, suffering from this preventable condition [1]. Efforts to find a pharmacological treatment for obesity have thus far proved unsuccessful; therefore, at present, bariatric surgical interventions are recognised as the most effective treatment for severe obesity [2].
For those patients undergoing bariatric surgical procedures, it is important that they receive accurate nutritional assessment both before and after these interventions are performed. Current methods of nutritional assessment in bariatric patients are often subjective, dependent on effective patient recall, and, ultimately, do not reflect the dynamic changes in body composition that are known to occur.
Due to the limitations of existing methods of nutritional assessment in bariatric patients, there is a clear clinical need to investigate novel strategies to overcome these challenges. One such approach is the analysis of metabolites within exhaled breath. Several studies have reported a rise in the ketone body acetone that was associated with prolonged starvation during either the intraoperative or post-operative period [3,4,5,6,7,8]. Those studies that have investigated acetone as a marker of nutrition in patients undergoing surgery have done so either at the time of operative intervention or in the immediate post-operative period. Whether changes in nutrition that occur during the pre-operative and extended post-operative periods are associated with equivalent changes in exhaled acetone and other ketones, therefore, remains unknown.
We hypothesise that analysis of ketones within exhaled breath can be used as a non-invasive method of assessing and monitoring nutritional status in patients undergoing treatment for obesity. The aims of the present study were to determine changes in the exhaled ketone concentrations in patients undergoing dietary restriction and bariatric surgery and to correlate those changes to parameters of weight loss and existing markers of nutrition.
Methods
Subjects
The current prospective cross-sectional study was designed so that three independent groups of patient groups were recruited at different time points during the course of treatment for obesity. Study recruitment took place at Imperial Weight Centre (St Mary’s Hospital, Imperial College Healthcare NHS Trust, London, UK) between October 2015 and April 2017. The study time points were as follows: at initial presentation for consideration of suitability for bariatric surgery, on the morning of planned bariatric surgery following a pre-operative low carbohydrate diet, and at the time of routine follow-up > 3 months following surgery. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Eligibility for bariatric surgery was determined in accordance with regional National Health Service commissioning criteria: patients with BMI ≥ 35 kg/m2 with obesity-related medical comorbidities (resistant hypertension, type 2 diabetes mellitus, obstructive sleep apnoea, polycystic ovary syndrome). Prior to being scheduled for a bariatric surgical procedure, a comprehensive multidisciplinary review of all patients was conducted.
Breath Sample Collection
Breath samples were collected from patients within both the outpatient clinic and pre-anaesthetic waiting area. Prior to exhaled breath sampling, subjects were required to remain seated at rest for a minimum of 15 min.
End-expiratory breath samples were collected by first instructing subjects to inhale through their mouth and then to exhale via a disposable mouthpiece in to a single use 250 ml GastroCH4ECK® steel bag (Ardmore Healthcare Ltd., Middleton on Sea, UK). An exhaust port within the sample bag permitted the initial portion of each exhalation to be discarded. Patients were asked to indicate when they were approaching the terminal portion of their exhalation at which point a researcher sealed the exhaust port of the sample bag allowing collection of 250 ml end-tidal breath. Upon collection, breath sample bags were sealed both by a one-way valve within the mouthpiece in addition to specially designed caps and compression clips. After being taught, the appropriate technique patients were given the opportunity to provide a practice breath sample before collection of a definitive sample. Prior to sample analysis, steel bags were transferred to an incubator held at a temperature of 37 °C in order to reduce internal condensation of water vapour.
Breath samples were analysed by a Profile-3 SIFT-MS (Instrument Science Ltd., Crewe, UK) which has been described previously in detail [9, 10]. For the purpose of this study, a targeted analysis was performed using the multiple ion monitoring mode of the SIFT-MS instrument using NO+ reagent ions (and their monohydrate), which have been shown to be suitable for the analysis of ketones [11]. Thus, acetone, 2-butanone, pentanone, hexanone, heptanone, and hexanone were measured in the breath samples. The count rates of the NO+ reagent ions and analyte ions for each ketone were integrated over a 60-s scan period. From these count rates and other physical parameters, including the breath gas sample flow rate, the concentrations of each ketone (all possible isomers) were calculated [12].
Subject Demographics and Metadata
For each subject, detailed demographics and related metadata were collected at the time of breath sample collection. Variables collected included the following: age, gender, body weight (pre-diet, pre-surgery, and post-surgery where appropriate), BMI (pre-diet, pre-surgery, and post-surgery where appropriate), excess body weight (EBW, pre-diet, pre-surgery, and post-surgery where appropriate), comorbidities, medications, time of last oral intake, time since surgery, post-operative complications, post-operative resolution of existing comorbidity (diabetes, hypertension, dyslipidaemia), and haematological and biochemical markers (neutrophil count, albumin, glucose, total cholesterol, triglycerides, high-density lipoprotein, low-density lipoprotein). Excess body weight was determined by subtracting patient’s ideal body weight from their recorded weight. Ideal body weight was determined using the Devine formula [13].
Pre-operative Low-Carbohydrate Diet
As part of a standard pre-operative pathway, all patients were assessed by a specialist obesity dietician and were provided with appropriate dietary advice. Prior to surgery, patients were asked to adhere to low carbohydrate (≤ 100 g/day carbohydrate; 800–1000 kcal/day) liver-shrinking diet for a period of 2–4 weeks (dependent on the patients’ BMI and gender).
Bariatric Surgical Procedures
All surgical procedures were performed laparoscopically by a consultant surgeon at the Imperial Weight Centre. Sleeve gastrectomy was performed after using a linear stapler with Seamguard® (GORE®) staple line reinforcement after a 34-F orogastric tube was inserted for the purpose of sizing the residual stomach. Antecolic–antegastric Roux-en-Y gastric bypass was performed using an end-to-side linear-stapled gastrojejunal anastomosis with biliopancreatic limb and Roux limb lengths typically 50 and 100 cm respectively.
Study Outcomes
The primary outcome of this study was to determine whether exhaled ketone concentrations significantly altered by either low-carbohydrate diet and/or bariatric surgery. Secondary outcomes were to determine whether exhaled ketone concentrations correlated with existing markers of nutrition, including BMI, EBW, and biochemical parameters, and to determine whether the surgical procedure influenced post-operative exhaled ketone concentrations.
Statistical Analysis
Data was extracted from the Profile-3 SIFT-MS software and exported to a Microsoft Office 2011 Excel file (Microsoft Corp., Redmond, WA, USA) wherein descriptive analysis was performed. Detailed statistical analysis was performed using SPSS Version 24.0 (IBM Corp., Armonk, New York, USA). Exhaled ketone concentrations (not normally distributed) are presented as median values with their associated interquartile range. Unless otherwise stated, all other values are presented as mean ± standard deviation. Ketone concentrations across each of the subject groups were initially compared using the Kruskal–Wallis test. All other pairwise comparisons were performed using either an independent sample Student’s t test or Mann–Whitney U test. Correlation of ketone concentrations to demographic and biochemical variables was conducted by Spearman’s rank correlation coefficient. Multivariate linear regression was performed to determine factors that were predicative of patients’ BMI and EBW at the time of sampling. Clinically relevant independent variables were included in the model using a forward stepwise selection procedure. Statistical significance was assumed for two-tailed P values < 0.05.
Results
Patient Demographics and Post-operative Outcomes
A total of 120 patients were recruited to this study, including 40 pre-diet, 40 post-diet (pre-operative), and 40 following either Roux-en-Y gastric bypass or sleeve gastrectomy. Patient demographics and post-operative outcomes are presented in Table 1. Study groups were well matched for patients’ age and gender. There was, however, significant variation in the American Society of Anesthesiologists (ASA) grade for patients within each group (P < 0.001), with a greater proportion of patients being ASA grade 1 in the post-operative group, reflecting post-procedural improvement in comorbidity rates. Post-operative patients were recruited a median of 12 (range, 4 to 27) months following surgery.
The pre-diet (baseline) weight (P = 0.418), BMI (P = 0.459), and EBW (P = 0.379) for patients within each of the sample groups were comparable (online supplementary file). All patients in the post-diet group reported compliance with the pre-operative low-carbohydrate diet. Of the 40 patients who underwent pre-operative dietary modification, 35 patients either lost or maintained their weight, whilst five patients exhibited minor weight increase. All patients lost weight following either Roux-en-Y gastric bypass or sleeve gastrectomy. Details of the effects of pre-operative dieting, Roux-en Y gastric bypass, and sleeve gastrectomy on patients’ weight and BMI for each patient group are presented online as a supplementary file.
Influence of Pre-operative Low-Carbohydrate Diet and Bariatric Surgery on Exhaled Ketone Concentrations
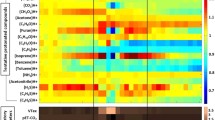
Breath sample collection was performed successfully without adverse event in all 120 patients. Exhaled acetone varied significantly between each of the three study groups, with higher concentrations observed in patients following pre-operative diet and bariatric surgery (P < 0.001) (Table 2). In comparison, heptanone (P = 0.021) and octanone (P = 0.021) were observed at lower concentrations in the exhaled breath of patients following pre-operative diet and bariatric surgery. As no significant variation in exhaled butanone, pentanone, and hexanone concentrations was observed between study groups, these compounds were excluded from further analysis. It is noted that the standard error of the measurement of higher order ketones (butanone, ± 45%; pentanone, ± 44%; hexanone, ± 48%; heptanone, ± 39%; octanone, ± 53%) is proportionally greater than that observed for acetone (± 7%).
Correlation of Exhaled Ketones to Clinical Variables
Exhaled heptanone (ρ − 0.242, P = 0.009) correlated with patients’ age whilst acetone (ρ − 0.264, P = 0.005) and octanone (ρ 0.215, P = 0.022) were also observed to correlate with EBW.
Comparison of biochemical parameters between the three patient groups revealed significant variation in the neutrophil count (P < 0.001), glucose (P = 0.001), low-density lipoprotein (P = 0.016), and triglyceride (P = 0.045) (Table 3). Acetone concentration demonstrated a significant correlation with high-density lipoprotein (ρ 0.331, P = 0.002) as well as an inverse correlation with neutrophil count (ρ − 0.282, P = 0.004), triglyceride (ρ − 0.300, P = 0.006), glucose (ρ − 0.306, P = 0.017), and total cholesterol (ρ − 0.259, P = 0.019). Octanone was observed to correlate with neutrophil count (ρ 0.261, P = 0.008) and triglyceride (ρ 0.258, P = 0.019).
When each patient group was considered independently, a diagnosis of type 2 diabetes did not significantly influence exhaled acetone, heptanone, and octanone concentrations (P > 0.05).
Multivariate Linear Regression of Factors Predictive of Patients’ EBW
Multivariate linear regression was performed to determine demographic and biochemical factors that were predicative of patients’ EBW at the time of assessment. Findings demonstrated that neutrophil count, glucose, acetone, and low-density lipoprotein concentration explained a significant amount of variation in patients’ EBW (F(df 3, 43) = 7.4, P = 0.0001, R2 = 0.41, R2 adjusted = 0.36). With the exception of glucose (Beta = 0.24, t(46) = 2.00, P = 0.053), each of these variables significantly predicted EBW within the model: neutrophil count (Beta = 0.41, t(46) = 3.39, P = 0.002), acetone (Beta = − 0.34, t(46) = − 2.78, P = 0.008), and low-density lipoprotein (Beta = − 0.30, t(46) = 2.42, P = 0.020).
Influence of Surgical Approach
Of those patients recruited to the post-operative group, 15 underwent Roux-en-Y gastric bypass compared to 25 who underwent sleeve gastrectomy. When considered separately, these patient groups were well matched for demographic and perioperative variables (Table 4). Breath analysis was performed a median of 12 months from the time of surgery in both groups of patients (P = 0.200). Comparison of EBW and percentage loss of EBW at the time of sampling likewise showed statistical equivalence (P > 0.05).
Acetone concentrations tended to be higher in the exhaled breath of patients who underwent sleeve gastrectomy (1850 ppb, 1460–2678) compared to patients who underwent Roux-en-Y gastric bypass (1523 ppb, 995–1968), although the difference did not reach statistical significance (P = 0.495). Similarly, no difference was observed in heptanone and octanone concentrations between surgical groups (P > 0.05). Exhaled acetone, heptanone, and octanone concentration was not significantly correlated to the time elapsed since surgery (P > 0.05).
Discussion
Ketosis occurs in all humans and is a critical part of energy metabolism, influenced by dietary intake, body composition, and the presence of disease states, including diabetes. Unlike glycolysis, which is dependent on glucose as its source of energy, ketosis relies on the breakdown of adipose tissue to produce free fatty acids that are metabolised by the liver to acetyl-CoA and subsequently to ketone bodies, including acetoacetate, β-hydroxybutyrate, and acetone. Of these three ketone bodies, acetone, due to its small molecular weight, can readily diffuse into the airspaces of the lung, thus permitting its detection in exhaled breath. Whilst several other ketones were detected within exhaled breath, pathways for their endogenous production and excretion in exhaled breath are less clear.
As well as being associated with the duration of fasting and consumption of a ketogenic diet [14], several authors have investigated the role of exhaled acetone as a marker of fat loss [15]. Kundu et al. identified that in overweight subjects restricted to a low-calorie diet (1200 kcal/day, ≤ 40 g fat, and ≤ 40 g carbohydrate), fat loss was directly proportional to breath acetone concentration [15]. The same author confirmed these findings in patients who received a low-calorie diet (high carbohydrate moderate protein and low fat) [16]. The addition of daily exercise to a low-calorie diet also appears to yield a further rise in acetone that is proportion to weight loss and to a lesser extent fat loss [15].
In the current study, acetone concentrations within exhaled breath were lowest in patients at the time of initial assessment prior to dietary and surgical intervention. This is in keeping with the finding that breath acetone is inversely proportional to patients’ BMI, reported herein and by previous studies [17, 18]. The additional finding that exhaled acetone was also inversely proportional to patients’ EBW is not unexpected in view the strong positive correlation that exists between BMI and EBW (ρ 0.979, P < 0.0001). Whilst it is noted that the median acetone concentration within the exhaled breath of obese patients at baseline in the current study is similar to that previously reported in healthy adult volunteers, a shorter period of pre-test fasting may explain the lower levels in the healthy population [19].
Explanation for the association between acetone production and excess body weight reflects a known resistance of obese patients to ketogenesis and fat loss that exists prior to and during periods of short-term dietary restriction [20, 21]. Patients who lost weight following dietary restriction and bariatric surgery in the current study had a corresponding rise in breath acetone concentration. It has been hypothesised that as obese patients begin to lose weight, both their rate of fat loss and concentration of breath acetone will increase [15]. Whilst it was possible in the current study to determine the degree of weight loss that patients experienced as a result of dietary restriction and/or bariatric surgery, it was not possible to determine either fat loss or change in breath acetone concentration from baseline. Accordingly, it is difficult to draw firm conclusions as to the relationship between changes in body composition and breath acetone in the current study.
In addition to patients’ BMI and EBW, breath acetone was correlated with several biochemical makers of nutrition and fat metabolism, including concentrations of high-density lipoprotein, neutrophil count, triglyceride, and glucose. These findings are in agreement with existing evidence documenting changes in lipid and glucose metabolism that are associated with obesity and weight loss [2, 22,23,24,25]. Multivariate linear regression revealed that a model incorporating neutrophil count, acetone, low-density lipoprotein and glucose, could predict 41% of the variance in EBW. The association of raised neutrophil count, low-density lipoprotein, and glucose with increased BMI/EBW is well established in the literature [2, 22, 24]. In the setting of obesity, increased numbers of white blood cells, including neutrophils, are thought to reflect the pro-inflammatory characteristics associated with this condition and its related comorbidities [24, 26]. Previous studies have observed a reduction in white blood cell count in response to progressive weight loss [24]. The association between obesity and elevated glucose and low-density lipoproteins is reflective of dyslipidaemia and insulin resistance, which are a major feature of this condition.
Of the other ketones analysed, heptanone, and octanone concentrations decreased with increasing weight loss. Furthermore, octanone concentrations were observed to positively correlate with EBW, neutrophil count, and triglyceride. However, as mentioned previously, it is important to note that whilst the acetone measurements are very reliable (estimated standard error ± 7%), other ketones, which are present at much lower concentrations in exhaled breath, are subject to a lower precision and proportionally greater standard error (typically ± 45%) in their measurement.
To our knowledge, this is the first study to report changes in exhaled ketones, other than acetone. Previous authors have, however, reported a decrease in urine total 4-heptanone in obese subjects who were fasting, reflecting the concurrent increase in lipolysis and fatty acid oxidation [27]. In an animal model, administration of 3-hepatanone was associated with weight gain [28]. However, the precise endogenous origins and clinical significance of hepatanone and other higher-order ketones remains unknown. Whilst higher order ketones have also been detected within urine headspace, it is unclear whether their concentrations correlated with those measured with exhaled breath [29]. To reiterate, these larger chain ketones appear in exhaled breath at relatively low concentrations and approach the detection limit of the current SIFT-MS instrument. It is nevertheless possible that these other ketones may serve to provide additional information as to the metabolic changes that occur at a result of weight loss surgery.
This study has a number of important limitations, including the lack of longitudinal data for breath ketones in individual patients at different stages of treatment. In the absence of such data, this study relies on the comparison of independent patient groups taken at a single time point during the course of their treatment. The opportunity to compare longitudinal data for patients throughout their treatment would permit more accurate correlation to changes in body composition and biochemical parameters. This may, in turn, support efforts to determine the role of breath ketones in predicating metabolic status and response to dietary and/or surgical therapy. In spite of this limitation, this study still represents the first concerted effort to determine the effects that surgical treatment of obesity has on exhaled ketone concentrations.
Future studies must now seek to establish the utility of exhaled ketones as a method of assessing the response to diet and bariatric surgery. Priority should be given to longitudinal studies. Such studies should seek to conduct serial measurements of breath ketones, blood and urine samples in combination with other methods of clinical and nutritional assessment. Further consideration should also be given to studies that aim to correlate breath ketones with measures of body composition, such as bioelectrical impedance analysis.
In conclusion, this is the first study to systematically explore variations in exhaled ketone concentrations in patients undergoing treatment for obesity. The most promising finding concerns the significant rise in acetone that was observed in patients following both dietary restriction and bariatric surgery. The observed variations in the concentrations of higher-order ketones, which are present at much lower concentrations, have not previously been reported and warrant further investigation. It is envisaged that the detection of ketones within exhaled breath may offer a promising method of non-invasive nutritional assessment in bariatric surgical patients.
References
WHO. Fact sheet: obesity and overweight, accessed on 12th September 2017 (http://www.who.int/mediacentre/factsheets/fs311/en/). 2016.
Colquitt JL, Pickett K, Loveman E, et al. Surgery for weight loss in adults. Cochrane Database Syst Rev. 2014;08(8):CD003641.
Boshier PR, Cushnir JR, Mistry V, et al. On-line, real time monitoring of exhaled trace gases by SIFT-MS in the perioperative setting: a feasibility study. Analyst. 2011;136(16):3233–7.
Boshier PR, Hanna GB, Marczin N. Exhaled nitric oxide as biomarker of acute lung injury: an unfulfilled promise? J Breath Res. 2013;7(1):017118.
Alexiou C, Tang AT, Sheppard SV, et al. A prospective randomized study to evaluate the effect of leukodepletion on the rate of alveolar production of exhaled nitric oxide during cardiopulmonary bypass. Ann Thorac Surg. 2004;78(6):2139–45. discussion 45
Dolch ME, Chouker A, Hornuss C, et al. Quantification of propionaldehyde in breath of patients after lung transplantation. Free Radic Biol Med. 2015;85:157–64.
Ross BM. Changes in oral trace gas concentrations following orthognathic surgery and intermaxillary fixation: a case study using selected ion flow tube mass spectrometry. Int J Oral Sci. 2011;3(3):160–4.
Kischkel S, Miekisch W, Fuchs P, et al. Breath analysis during one-lung ventilation in cancer patients. Eur Respir J. 2012;40(3):706–13.
Smith D, Spanel P. SIFT-MS and FA-MS methods for ambient gas phase analysis: developments and applications in the UK. Analyst. 2015;140(8):2573–91.
Smith D, Spanel P. Selected ion flow tube mass spectrometry (SIFT-MS) for on-line trace gas analysis. Mass Spectrom Rev. 2005;24(5):661–700.
Smith D, Wang T, Spanel P. Analysis of ketones by selected ion flow tube mass spectrometry. Rapid Commun Mass Spectrom. 2003;17(23):2655–60.
Spanel P, Dryahina K, Smith D. A general method for the calculation of absolute trace gas concentrations in air and breath from selected ion flow tube mass spectrometry data. Int J of Mass Spectrometry. 2006;249-250:230–9.
Devine BJ. Gentamicin therapy. Drug Intell Clin Pharm. 1974;8:650–5.
Spanel P, Dryahina K, Rejskova A, et al. Breath acetone concentration; biological variability and the influence of diet. Physiol Meas. 2011;32(8):N23–31.
Anderson JC. Measuring breath acetone for monitoring fat loss: review. Obesity (Silver Spring). 2015;23(12):2327–34.
Kundu SK, Bruzek JA, Nair R, et al. Breath acetone analyzer: diagnostic tool to monitor dietary fat loss. Clin Chem. 1993;39(1):87–92.
Toyooka T, Hiyama S, Yamada Y. A prototype portable breath acetone analyzer for monitoring fat loss. J Breath Res. 2013;7(3):036005.
Kinoyama M, Nitta H, Watanabe A, et al. Acetone and isoprene concentrations in exhaled breath in healthy subjects. J Health Sci. 2008;54:471–7.
Turner C, Spanel P, Smith D. A longitudinal study of ammonia, acetone and propanol in the exhaled breath of 30 subjects using selected ion flow tube mass spectrometry, SIFT-MS. Physiol Meas. 2006;27(4):321–37.
Mohammadiha H. Resistance to ketonuria and ketosis in obese subjects. Am J Clin Nutr. 1974;27(11):1212–3.
Kekwick A, Pawan GL, Chalmers TM. Resistance to ketosis in obese subjects. Lancet. 1959;2(7113):1157–9.
Cunha FM, Oliveira J, Preto J, et al. The effect of bariatric surgery type on lipid profile: an age, sex, body mass index and excess weight loss matched study. Obes Surg. 2016;26(5):1041–7.
Shige H, Nestel P, Sviridov D, et al. Effect of weight reduction on the distribution of apolipoprotein A-I in high-density lipoprotein subfractions in obese non-insulin-dependent diabetic subjects. Metabolism. 2000;49(11):1453–9.
Dixon JB, O'Brien PE. Obesity and the white blood cell count: changes with sustained weight loss. Obes Surg. 2006;16(3):251–7.
Rashid S, Genest J. Effect of obesity on high-density lipoprotein metabolism. Obesity (Silver Spring). 2007;15(12):2875–88.
Chen SB, Lee YC, Ser KH, et al. Serum C-reactive protein and white blood cell count in morbidly obese surgical patients. Obes Surg. 2009 Apr;19(4):461–6.
Liebich HM. Gas chromatographic—mass spectrometric determination of total 4-heptanone, a new marker in diabetes mellitus. J Chromatogr. 1983;273(1):67–75.
O'Donoghue JL, Krasavage WJ, DiVincenzo GD, et al. Further studies on ketone neurotoxicity and interactions. Toxicol Appl Pharmacol. 1984;72(2):201–9.
Wang T, Spanel P, Smith D. Selected ion flow tube mass spectrometry of 3-hydroxybutyric acid, acetone and other ketones in the headspace of aqueous solution and urine. Int J of Mass Spectrometry. 2008;272:78–85.
Acknowledgements
The results of this study were given as an oral presentation at the 22nd World Congress of IFSO 2017, London, UK.
The authors are grateful to Mrs. Zenia Alaestante RN for the assistance with the patient recruitment.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval and Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
The authors declare that they have no competing interests.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Boshier, P.R., Fehervari, M., Markar, S.R. et al. Variation in Exhaled Acetone and Other Ketones in Patients Undergoing Bariatric Surgery: a Prospective Cross-sectional Study. OBES SURG 28, 2439–2446 (2018). https://doi.org/10.1007/s11695-018-3180-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-018-3180-5