
Abstract
Purpose
Multipoint pacing (MPP) improves left ventricular (LV) electrical synchrony in cardiac resynchronization therapy (CRT). SyncAV automatically adjusts atrioventricular delay (AVD) according to intrinsic AV intervals and may further improve synchrony. Their combination has not been assessed. The objective was to evaluate the improvement in electrical synchrony achieved by SyncAV combined with MPP in an international, multicenter study.
Methods
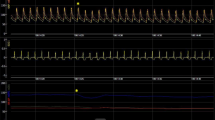
Patients with LBBB undergoing CRT implant with a quadripolar lead (Abbott Quartet™) were prospectively enrolled. QRS duration (QRSd) was measured by blinded observers from 12-lead ECG during: intrinsic conduction, BiV pacing (conventional biventricular pacing, nominal static AVD), MPP (2 LV cathodes maximally spaced, nominal static AVD), BiV + SyncAV, and MPP + SyncAV. All SyncAV offsets were individualized for each patient to yield the narrowest QRSd during BiV pacing. QRSd changes were compared by ANOVA and post hoc Tukey-Kramer tests.
Results
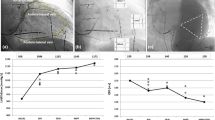
One hundred and three patients were enrolled (65.7 ± 12.1 years, 67% male, 37% ischemic, EF 26.4 ± 6.5%, PR 190.3 ± 39.1 ms). Relative to intrinsic conduction (QRSd of 165 ± 16 ms), BiV reduced QRSd by 11.9% to 145 ± 18 ms (P < 0.001 vs intrinsic), and MPP reduced QRSd by 13.3% to 142 ± 19 ms (P < 0.001 vs intrinsic). However, enabling SyncAV with a patient-optimized offset nearly doubled this QRSd reduction. BiV + SyncAV reduced QRSd by 22.0% to 128 ± 13 ms (P < 0.001 vs BiV), while MPP + SyncAV reduced QRSd further by 25.6% to 122 ± 14 ms (P < 0.05 vs BiV + SyncAV).
Conclusion
SyncAV can significantly improve acute electrical synchrony beyond conventional CRT, with further improvement achieved by superimposing MPP.





Similar content being viewed by others

Data availability
Not applicable
References
Sutton MGS, Plappert T, Abraham WT, Smith AL, DeLurgio DB, Leon AR, et al. Effect of cardiac resynchronization therapy on left ventricular size and function in chronic heart failure. Circulation. 2003;107:1985–90.
Cazeau S, Leclercq C, Lavergne T, Walker S, Varma C, Linde C, et al. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med. 2001;344:873–80.
Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, Loh E, et al. Cardiac resynchronization in chronic heart failure. N Engl J Med. 2002;346:1845–53.
Fornwalt BK, Sprague WW, BeDell P, Suever JD, Gerritse B, Merlino JD, et al. Agreement is poor among current criteria used to define response to cardiac resynchronization therapy. Circulation. 2010;121:1985–91.
Tolosana JM, Mont L. Cardiac resynchronization therapy - how to decrease nonresponders. Heart Fail Clin. 2017;13:233–40.
Ginks MR, Shetty AK, Lambiase PD, Duckett SG, Bostock J, Peacock JL, et al. Benefits of endocardial and multisite pacing are dependent on the type of left ventricular electric activation pattern and presence of ischemic heart disease: insights from electroanatomic mapping. Circ Arrhythm Electrophysiol. 2012;5:889–97.
Menardi E, Ballari GP, Goletto C, Rossetti G, Vado A. Characterization of ventricular activation pattern and acute hemodynamics during multipoint left ventricular pacing. Hear Rhythm. 2015;12:1762–9.
Varma N, Ploux S, Ritter P, Wilkoff B, Eschalier R, Bordachar P. Noninvasive mapping of electrical dyssynchrony in heart failure and cardiac resynchronization therapy. Card Electrophysiol Clin. 2015;7:125–34.
Ter Horst IAH, Bogaard MD, Tuinenburg AE, Mast TP, de Boer TP, Doevendans P, et al. The concept of triple wavefront fusion during biventricular pacing: using the EGM to produce the best acute hemodynamic improvement in CRT. Pacing Clin Electrophysiol. 2017;40:873–82.
Lunati M, Magenta G, Cattafi G, Moreo A, Falaschi G, Contardi D, et al. Clinical relevance of systematic CRT device optimization. J Atr Fibrillation. 2014;7:62–9.
Arbelo E, Tolosana JM, Trucco E, Penela D, Borras R, Doltra A, et al. Fusion-optimized intervals (FOI): a new method to achieve the narrowest QRS for optimization of the AV and VV intervals in patients undergoing cardiac resynchronization therapy. J Cardiovasc Electrophysiol. 2014;25:283–92.
Tamborero D, Vidal B, Tolosana JM, Sitges M, Berruezo A, Silva E, et al. Electrocardiographic versus echocardiographic optimization of the interventricular pacing delay in patients undergoing cardiac resynchronization therapy. J Cardiovasc Electrophysiol. 2011;22:1129–34.
Vatasescu R, Berruezo A, Mont L, Tamborero D, Sitges M, Silva E, et al. Midterm “super-response” to cardiac resynchronization therapy by biventricular pacing with fusion: insights from electro-anatomical mapping. Europace. 2009;11:1675–82.
Lecoq G, Leclercq C, Leray E, Crocq C, Alonso C, de PC, et al. Clinical and electrocardiographic predictors of a positive response to cardiac resynchronization therapy in advanced heart failure. Eur Heart J. 2005;26:1094–100.
Trucco E, Tolosana JM, Arbelo E, Doltra A, Castel A, Benito E, et al. Improvement of reverse remodeling using ECG fusion-optimized intervals in cardiac resynchronization therapy: a randomized study. JACC Clin Electrophysiol. 2017.
AlTurki A, Lima PY, Garcia D, Montemezzo M, Al-Dosari A, Vidal A, et al. Cardiac resynchronization therapy reprogramming to improve electrical synchrony in patients with existing devices. J Electrocardiol. 2019;56:94–9. https://doi.org/10.1016/j.jelectrocard.2019.07.008.
Varma N, O’Donnell D, Bassiouny M, Ritter P, Pappone C, Mangual J, et al. Programming cardiac resynchronization therapy for electrical synchrony: reaching beyond left bundle branch block and left ventricular activation delay. J Am Heart Assoc. 2018;7:e007489. https://doi.org/10.1161/JAHA.117.007489.
Thibault B, Ritter P, Bode K, Calo L, Mondesert B, Mangual JO, et al. Dynamic programming of atrioventricular delay improves electrical synchrony in a multicenter cardiac resynchronization therapy study. Hear Rhythm. 2019;16:1047–56. https://doi.org/10.1016/j.hrthm.2019.01.020.
Zanon F, Baracca E, Pastore G, Marcantoni L, Fraccaro C, Lanza D, et al. Multipoint pacing by a left ventricular quadripolar lead improves the acute hemodynamic response to CRT compared with conventional biventricular pacing at any site. Hear Rhythm. 2015;12:975–81.
Surawicz B, Childers R, Deal BJ, Gettes LS, Bailey JJ, Gorgels A, et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part III: intraventricular conduction disturbances: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee. Circulation. 2009;119:e235–40.
Thibault B, Dubuc M, Khairy P, Guerra PG, Macle L, Rivard L, et al. Acute haemodynamic comparison of multisite and biventricular pacing with a quadripolar left ventricular lead. Europace. 2013;15:984–91.
Pappone C, Calovic Z, Vicedomini G, Cuko A, McSpadden LC, Ryu K, et al. Multipoint left ventricular pacing improves acute hemodynamic response assessed with pressure-volume loops in cardiac resynchronization therapy patients. Hear Rhythm. 2014;11:394–401.
Osca J, Alonso P, Cano O, Andres A, Miro V, Tello MJ, et al. The use of multisite left ventricular pacing via quadripolar lead improves acute haemodynamics and mechanical dyssynchrony assessed by radial strain speckle tracking: initial results. Europace. 2015;18:560–7. https://doi.org/10.1093/europace/euv211.
Pappone C, Calovic Z, Vicedomini G, Cuko A, McSpadden LC, Ryu K, et al. Improving cardiac resynchronization therapy response with multipoint left ventricular pacing: twelve-month follow-up study. Hear Rhythm. 2015;12:1250–8.
Forleo GB, Santini L, Giammaria M, Potenza D, Curnis A, Calabrese V, et al. Multipoint pacing via a quadripolar left-ventricular lead: preliminary results from the Italian registry on multipoint left-ventricular pacing in cardiac resynchronization therapy (IRON-MPP). Europace. 2017;19:1170–7.
Zanon F, Marcantoni L, Baracca E, Pastore G, Lanza D, Fraccaro C, et al. Optimization of left ventricular pacing site plus multipoint pacing improves remodeling and clinical response to cardiac resynchronization therapy at 1 year. Hear Rhythm. 2016;13:1644–51. https://doi.org/10.1016/j.hrthm.2016.05.015.
Rickard J, Popovic Z, Verhaert D, Sraow D, Baranowski B, Martin DO, et al. The QRS narrowing index predicts reverse left ventricular remodeling following cardiac resynchronization therapy. Pacing Clin Electrophysiol. 2011;34:604–11.
Molhoek SG, Van EL, Bootsma M, Steendijk P, van der Wall EE, Schalij MJ. QRS duration and shortening to predict clinical response to cardiac resynchronization therapy in patients with end-stage heart failure. Pacing Clin Electrophysiol. 2004;27:308–13.
Funding
This study was funded by the Abbott.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All patients provided informed consent, and study protocols were approved by the ethics committee of each institution.
Conflict of interest
David O’Donnell received research grants and/or consultancy fees from Abbott, Boston Scientific, Biotronik, and Medtronic. Carlo Pappone and Bernard Thibault received research grants and/or consultancy fees from Abbott. Tim R. Betts has received research grants and/or consultancy fees from Abbott Medical, Boston Scientific, and Acutus Medical. Niraj Varma received research grants and/or consultancy fees from Abbott, Boston Scientific, Biotronik, and Medtronic. Brian Wisnoskey, Nima Badie, Lisa Odgers, Jan O. Mangual, Gary Cranke, Luke C. McSpadden, and Kyungmoo Ryu are Abbott employees. Taylah Smart, Michelle Ord, Tina Lin, Valter Bianchi, Antonio D’Onofrio, Leonardo Calò, and Anthony Chow have nothing to disclose.
Code availability
Not applicable
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
O’Donnell, D., Wisnoskey, B., Badie, N. et al. Electrical synchronization achieved by multipoint pacing combined with dynamic atrioventricular delay. J Interv Card Electrophysiol 61, 453–460 (2021). https://doi.org/10.1007/s10840-020-00842-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-020-00842-7