
Abstract
Purpose
There is still a significant amount of patients who do not sufficiently respond to cardiac resynchronization therapy (CRT). Previous studies demonstrated that the amount of dyssynchronous myocardium was predictive of response to CRT. Otherwise, non-response is frequently associated with high amounts of scar tissue. The combination of these parameters might yield a more accurate prediction of response. We hypothesized that the probability of a CRT response increases with the presence of high amounts of “viable and dyssynchronous” myocardium.
Methods
A total of 19 patients (17 male, 61 ± 10 years) underwent ECG-gated [18F]fluorodeoxyglucose (FDG) myocardial positron emission tomography (PET) before CRT device implantation and were followed for 6 months. Response to CRT was defined as clinical improvement of at least one New York Heart Association (NYHA) class in combination with left ventricular (LV) ejection fraction (EF) improvement of >5 %. Twelve responders (71 %) and seven non-responders (29 %) were identified. For each patient bullseye maps of FDG uptake and phase analysis were calculated (QPS/QGS 2012, Cedars-Sinai, Los Angeles, CA, USA) and fused. Amounts of myocardium representing “viable and synchronous”, “scar and synchronous”, viable and dyssynchronous or “scar and dyssynchronous” myocardium were quantified by planimetric measurements of the fused bullseye maps.
Results
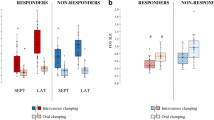
Responders by definition showed significant decrease in NYHA class and significant increase of LVEF. Furthermore, a significantly higher amount of viable and dyssynchronous myocardium was found as compared to non-responders (21 ± 13 % vs 6 ± 5 %; p < 0.05).
Conclusion
Combined assessment of myocardial viability and LV dyssynchrony is feasible using multiparametric [18F]FDG PET and could improve conventional response prediction criteria for CRT.


Similar content being viewed by others

Abbreviations
- CRT:
-
Cardiac resynchronization therapy
- LBBB:
-
Left bundle branch block
- LVEF:
-
Left ventricular ejection fraction
- LVESV:
-
Left ventricular end-systolic volume
- FDG:
-
Fluorodeoxyglucose
- PET:
-
Positron emission tomography
- CT:
-
Computed tomography
- SD:
-
Standard deviation
- VS:
-
Viable and synchronous
- VD:
-
Viable and dyssynchronous
- NVS:
-
Non-viable and synchronous
- NVD:
-
Non-viable and dyssynchronous
- LVEDD:
-
Left ventricular end-diastolic diameter
- LVEDV:
-
Left ventricular end-diastolic volume
References
McMurray JJV, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J 2012;33:1787–847.
Holzmeister J, Leclercq C. Implantable cardioverter defibrillators and cardiac resynchronisation therapy. Lancet 2011;378:722–30.
Tang ASL, Wells GA, Talajic M, Arnold MO, Sheldon R, Connolly S, et al. Cardiac-resynchronization therapy for mild-to-moderate heart failure. N Engl J Med 2010;363:2385–95.
Cleland JGF, Daubert J-C, Erdmann E, Freemantle N, Gras D, Kappenberger L, et al. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med 2005;352:1539–49.
Tang WHW, Boehmer J, Gras D. Multispecialty approach: the need for heart failure disease management for refining cardiac resynchronization therapy. Heart Rhythm 2012;9(8 Suppl):S45–50.
Birnie DH, Tang AS. The problem of non-response to cardiac resynchronization therapy. Curr Opin Cardiol 2006;21:20–6.
Xu Y-Z, Cha Y-M, Feng D, Powell BD, Wiste HJ, Hua W, et al. Impact of myocardial scarring on outcomes of cardiac resynchronization therapy: extent or location? J Nucl Med 2012;53:47–54.
van Campen CMC, Visser FC, van der Weerdt AP, Knaapen P, Comans EFI, Lammertsma AA, et al. FDG PET as a predictor of response to resynchronisation therapy in patients with ischaemic cardiomyopathy. Eur J Nucl Med Mol Imaging 2007;34:309–15.
Chalil S, Stegemann B, Muhyaldeen SA, Khadjooi K, Foley PW, Smith REA, et al. Effect of posterolateral left ventricular scar on mortality and morbidity following cardiac resynchronization therapy. Pacing Clin Electrophysiol 2007;30:1201–9.
Uebleis C, Ulbrich M, Tegtmeyer R, Schuessler F, Haserueck N, Siebermair J, et al. Electrocardiogram-gated 18F-FDG PET/CT hybrid imaging in patients with unsatisfactory response to cardiac resynchronization therapy: initial clinical results. J Nucl Med 2010;52:67–71.
Boogers MM, Van Kriekinge SD, Henneman MM, Ypenburg C, Van Bommel RJ, Boersma E, et al. Quantitative gated SPECT-derived phase analysis on gated myocardial perfusion SPECT detects left ventricular dyssynchrony and predicts response to cardiac resynchronization therapy. J Nucl Med 2009;50:718–25.
Adelstein EC, Saba S. Scar burden by myocardial perfusion imaging predicts echocardiographic response to cardiac resynchronization therapy in ischemic cardiomyopathy. Am Heart J 2007;153:105–12.
Bax JJ, Marwick TH, Molhoek SG, Bleeker GB, van Erven L, Boersma E, et al. Left ventricular dyssynchrony predicts benefit of cardiac resynchronization therapy in patients with end-stage heart failure before pacemaker implantation. Am J Cardiol 2003;92:1238–40.
Henneman MM, Chen J, Dibbets-Schneider P, Stokkel MP, Bleeker GB, Ypenburg C, et al. Can LV dyssynchrony as assessed with phase analysis on gated myocardial perfusion SPECT predict response to CRT? J Nucl Med 2007;48:1104–11.
Ypenburg C, Schalij MJ, Bleeker GB, Steendijk P, Boersma E, Dibbets-Schneider P, et al. Extent of viability to predict response to cardiac resynchronization therapy in ischemic heart failure patients. J Nucl Med 2006;47:1565–70.
Dilsizian V, Bacharach SL, Beanlands RS, Bergmann SR, Delbeke D, Gropler RJ, et al. PET myocardial perfusion and metabolism clinical imaging. J Nucl Cardiol 2009;16:651.
Schinkel AFL, Bax JJ, Biagini E, Elhendy A, van Domburg RT, Valkema R, et al. Myocardial technetium-99m-tetrofosmin single-photon emission computed tomography compared with 18F-fluorodeoxyglucose imaging to assess myocardial viability. Am J Cardiol 2005;95:1223–5.
Chen J, Garcia EV, Folks RD, Cooke CD, Faber TL, Tauxe EL, et al. Onset of left ventricular mechanical contraction as determined by phase analysis of ECG-gated myocardial perfusion SPECT imaging: development of a diagnostic tool for assessment of cardiac mechanical dyssynchrony. J Nucl Cardiol 2005;12:687–95.
Brambatti M, Guerra F, Matassini MV, Cipolletta L, Barbarossa A, Urbinati A, et al. Cardiac resynchronization therapy improves ejection fraction and cardiac remodelling regardless of patients’ age. Europace 2013;15:704–10.
Prinz C, Lehmann R, Schwarz M, Prinz E-M, Bitter T, Vogt J, et al. Left ventricular dyssynchrony predicts clinical response to CRT - a long-term follow-up single-center prospective observational cohort study. Echocardiography 2013. doi:10.1111/echo.12165.
Bonow RO, Maurer G, Lee KL, Holly TA, Binkley PF, Desvigne-Nickens P, et al. Myocardial viability and survival in ischemic left ventricular dysfunction. N Engl J Med 2011;364:1617–25.
Riedlbauchová L, Brunken R, Jaber WA, Popová L, Patel D, Lánská V, et al. The impact of myocardial viability on the clinical outcome of cardiac resynchronization therapy. J Cardiovasc Electrophysiol 2009;20:50–7.
Murphy RT, Sigurdsson G, Mulamalla S, Agler D, Popovic ZB, Starling RC, et al. Tissue synchronization imaging and optimal left ventricular pacing site in cardiac resynchronization therapy. Am J Cardiol 2006;97:1615–21.
Ypenburg C, van Bommel RJ, Delgado V, Mollema SA, Bleeker GB, Boersma E, et al. Optimal left ventricular lead position predicts reverse remodeling and survival after cardiac resynchronization therapy. J Am Coll Cardiol 2008;52:1402–9.
Uebleis C, Hellweger S, Laubender RP, Becker A, Sohn H-Y, Lehner S, et al. Left ventricular dyssynchrony assessed by gated SPECT phase analysis is an independent predictor of death in patients with advanced coronary artery disease and reduced left ventricular function not undergoing cardiac resynchronization therapy. Eur J Nucl Med Mol Imaging 2012;39:1561–9.
Pazhenkottil AP, Buechel RR, Nkoulou R, Ghadri J-R, Herzog BA, Husmann L, et al. Left ventricular dyssynchrony assessment by phase analysis from gated PET-FDG scans. J Nucl Cardiol 2011;18:920–5.
Leclercq C, Faris O, Tunin R, Johnson J, Kato R, Evans F, et al. Systolic improvement and mechanical resynchronization does not require electrical synchrony in the dilated failing heart with left bundle-branch block. Circulation 2002;106:1760–3.
Conflicts of interest
Cedars-Sinai Medical Center receives royalties for the licensure of software used in the quantitative assessment of function, perfusion and viability, a portion of which is distributed to some of the authors of this article.
Author information
Authors and Affiliations
Corresponding author
Additional information
Sebastian Lehner and Christopher Uebleis contributed equally to this work
Rights and permissions
About this article
Cite this article
Lehner, S., Uebleis, C., Schüßler, F. et al. The amount of viable and dyssynchronous myocardium is associated with response to cardiac resynchronization therapy: initial clinical results using multiparametric ECG-gated [18F]FDG PET. Eur J Nucl Med Mol Imaging 40, 1876–1883 (2013). https://doi.org/10.1007/s00259-013-2516-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-013-2516-6