
Abstract
Summary
People with spinal cord injury (SCI) lose bone and muscle integrity after their injury. Early doses of stress, applied through electrically induced muscle contractions, preserved bone density at high-risk sites. Appropriately prescribed stress early after the injury may be an important consideration to prevent bone loss after SCI.
Introduction
Skeletal muscle force can deliver high compressive loads to bones of people with spinal cord injury (SCI). The effective osteogenic dose of load for the distal femur, a chief site of fracture, is unknown. The purpose of this study is to compare three doses of bone compressive loads at the distal femur in individuals with complete SCI who receive a novel stand training intervention.
Methods
Seven participants performed unilateral quadriceps stimulation in supported stance [150% body weight (BW) compressive load—“High Dose” while opposite leg received 40% BW—“Low Dose”]. Five participants stood passively without applying quadriceps electrical stimulation to either leg (40% BW load—“Low Dose”). Fifteen participants performed no standing (0% BW load—“Untrained”) and 14 individuals without SCI provided normative data. Participants underwent bone mineral density (BMD) assessment between one and six times over a 3-year training protocol.
Results
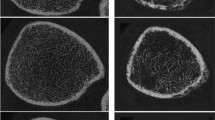
BMD for the High Dose group significantly exceeded BMD for both the Low Dose and the Untrained groups (p < 0.05). No significant difference existed between the Low Dose and Untrained groups (p > 0.05), indicating that BMD for participants performing passive stance did not differ from individuals who performed no standing. High-resolution CT imaging of one High Dose participant revealed 86% higher BMD and 67% higher trabecular width in the High Dose limb.
Conclusion
Over 3 years of training, 150% BW compressive load in upright stance significantly attenuated BMD decline when compared to passive standing or to no standing. High-resolution CT indicated that trabecular architecture was preserved by the 150% BW dose of load.






Similar content being viewed by others


References
Eser P, Frotzler A, Zehnder Y, Wick L, Knecht H, Denoth J, Schiessl H (2004) Relationship between the duration of paralysis and bone structure: a pQCT study of spinal cord injured individuals. Bone 34:869–880
Fattal C, Mariano-Goulart D, Thomas E, Rouays-Mabit H, Verollet C, Maimoun L (2011) Osteoporosis in persons with spinal cord injury: the need for a targeted therapeutic education. Arch Phys Med Rehabil 92:59–67
Lanyon LE (1996) Using functional loading to influence bone mass and architecture: objectives, mechanisms, and relationship with estrogen of the mechanically adaptive process in bone. Bone 18:37S–43S
Davis GM, Hamzaid NA, Fornusek C (2008) Cardiorespiratory, metabolic, and biomechanical responses during functional electrical stimulation leg exercise: health and fitness benefits. Artif Organs 32:625–629
Ben M, Harvey L, Denis S, Glinsky J, Goehl G, Chee S, Herbert RD (2005) Does 12 weeks of regular standing prevent loss of ankle mobility and bone mineral density in people with recent spinal cord injuries? Aust J Physiother 51:251–256
Clark JM, Jelbart M, Rischbieth H, Strayer J, Chatterton B, Schultz C, Marshall R (2007) Physiological effects of lower extremity functional electrical stimulation in early spinal cord injury: lack of efficacy to prevent bone loss. Spinal Cord 45:78–85
Giangregorio LM, Hicks AL, Webber CE, Phillips SM, Craven BC, Bugaresti JM, McCartney N (2005) Body weight supported treadmill training in acute spinal cord injury: impact on muscle and bone. Spinal Cord 43:649–657
Leeds EM, Klose KJ, Ganz W, Serafini A, Green BA (1990) Bone mineral density after bicycle ergometry training. Arch Phys Med Rehabil 71:207–209
BeDell KK, Scremin AM, Perell KL, Kunkel CF (1996) Effects of functional electrical stimulation-induced lower extremity cycling on bone density of spinal cord-injured patients. Am J Phys Med Rehabil 75:29–34
Frost HM (2003) Bone’s mechanostat: a 2003 update. Anat Rec 275A:1081–1101
Bloomfield SA, Mysiw WJ, Jackson RD (1996) Bone mass and endocrine adaptations to training in spinal cord injured individuals. Bone 19:61–68
Frotzler A, Coupaud S, Perret C, Kakebeeke TH, Hunt KJ, Donaldson Nde N, Eser P (2008) High-volume FES-cycling partially reverses bone loss in people with chronic spinal cord injury. Bone 43:169–176
Mohr T, Podenphant J, Biering-Sorensen F, Galbo H, Thamsborg G, Kjaer M (1997) Increased bone mineral density after prolonged electrically induced cycle training of paralyzed limbs in spinal cord injured man. Calcif Tissue Int 61:22–25
Snyder WS (ed) (1975) Report of the task group on reference man. Pergamon, Oxford
Eser P, Frotzler A, Zehnder Y, Denoth J (2005) Fracture threshold in the femur and tibia of people with spinal cord injury as determined by peripheral quantitative computed tomography. Arch Phys Med Rehabil 86:498–504
Shields RK, Dudley-Javoroski S (2006) Musculoskeletal plasticity after acute spinal cord injury: effects of long-term neuromuscular electrical stimulation training. J Neurophysiol 95:2380–2390
Shields RK, Dudley-Javoroski S, Frey Law L (2006) Electrically-induced muscle contractions influence bone density decline after spinal cord injury. Spine 31:548–553
Shields RK, Dudley-Javoroski S, Littmann AE (2006) Post-fatigue potentiation of paralyzed soleus muscle: evidence for adaptation with long-term electrical stimulation training. J Appl Physiol 101:556–565
Shields RK, Dudley-Javoroski S (2006) Musculoskeletal adaptation in chronic spinal cord injury: effects of long-term soleus electrical stimulation training. J Neurorehabil Neural Repair 21:169–179
Dudley-Javoroski S, Shields RK (2008) Asymmetric bone adaptations to soleus mechanical loading after spinal cord injury. J Musculoskelet Neuronal Interact 8:227–238
Zioupos P, Gresle M, Winwood K (2008) Fatigue strength of human cortical bone: age, physical, and material heterogeneity effects. J Biomed Mater Res A 86:627–636
Dudley-Javoroski S, Littmann AE, Chang SH, McHenry CL, Shields RK (2011) Enhancing muscle force and femur compressive loads via feedback-controlled stimulation of paralyzed quadriceps in humans. Arch Phys Med Rehabil 92:242–249
Shields RK, Dudley-Javoroski S (2005) Monitoring standing wheelchair use after spinal cord injury: a case report. Disabil Rehabil 27:142–146
American Spinal Injury Association (2002) International standards for neurological classification of SCI. American Spinal Injury Association, Atlanta
Frey Law L, Shields RK (2004) Femoral loads during passive, active, and active-resistive stance after spinal cord injury: a mathematical model. Clin Biomech 19:313–321
Dudley-Javoroski S, Shields RK (2008) Dose estimation and surveillance of mechanical loading interventions for bone loss after spinal cord injury. Phys Ther 88:387–396
Dudley-Javoroski S, Shields RK (2010) Longitudinal changes in femur bone mineral density after spinal cord injury: effects of slice placement and peel method. Osteoporos Int 21:985–995
Shields RK, Dudley-Javoroski S, Boaldin KM, Corey TA, Fog DB, Ruen JM (2006) Peripheral quantitative computed tomography: measurement sensitivity in persons with and without spinal cord injury. Arch Phys Med Rehabil 87:1376–1381
Hangartner TN, Gilsanz V (1996) Evaluation of cortical bone by computed tomography. J Bone Miner Res 11:1518–1525
Saha PK, Xu Y, Duan H, Heiner A, Liang G (2010) Volumetric topological analysis: a novel approach for trabecular bone classification on the continuum between plates and rods. IEEE Trans Med Imaging 29:1821–1838
Wehrli FW, Ladinsky GA, Jones C et al (2008) In vivo magnetic resonance detects rapid remodeling changes in the topology of the trabecular bone network after menopause and the protective effect of estradiol. J Bone Miner Res 23:730–740
Eser P, Schiessl H, Willnecker J (2004) Bone loss and steady state after spinal cord injury: a cross-sectional study using pQCT. J Musculoskelet Neuronal Interact 4:197–198
Frotzler A, Berger M, Knecht H, Eser P (2008) Bone steady-state is established at reduced bone strength after spinal cord injury: a longitudinal study using peripheral quantitative computed tomography (pQCT). Bone 43:549–555
Lai CH, Chang WH, Chan WP, Peng CW, Shen LK, Chen JJ, Chen SC (2010) Effects of functional electrical stimulation cycling exercise on bone mineral density loss in the early stages of spinal cord injury. J Rehabil Med 42:150–154
Lauer RT, Smith BT, Mulcahey MJ, Betz RR, Johnston TE (2011) Effects of cycling and/or electrical stimulation on bone mineral density in children with spinal cord injury. Spinal Cord 49:917–923
Ashe MC, Eng JJ, Krassioukov AV, Warburton DE, Hung C, Tawashy A (2010) Response to functional electrical stimulation cycling in women with spinal cord injuries using dual-energy X-ray absorptiometry and peripheral quantitative computed tomography: a case series. J Spinal Cord Med 33:68–72
Eser P, de Bruin ED, Telley I, Lechner HE, Knecht H, Stussi E (2003) Effect of electrical stimulation-induced cycling on bone mineral density in spinal cord-injured patients. Eur J Clin Investig 33:412–419
Groah SL, Lichy AM, Libin AV, Ljungberg I (2010) Intensive electrical stimulation attenuates femoral bone loss in acute spinal cord injury. PM&R 2:1080–1087
Belanger M, Stein RB, Wheeler GD, Gordon T, Leduc B (2000) Electrical stimulation: can it increase muscle strength and reverse osteopenia in spinal cord injured individuals? Arch Phys Med Rehabil 81:1090–1098
Hartkopp A, Murphy RJ, Mohr T, Kjaer M, Biering-Sorensen F (1998) Bone fracture during electrical stimulation of the quadriceps in a spinal cord injured subject. Arch Phys Med Rehabil 79:1133–1136
Alekna V, Tamulaitiene M, Sinevicius T, Juocevicius A (2008) Effect of weight-bearing activities on bone mineral density in spinal cord injured patients during the period of the first two years. Spinal Cord 46:727–732
Dionyssiotis Y, Lyritis GP, Mavrogenis AF, Papagelopoulos PJ (2011) Factors influencing bone loss in paraplegia. Hippokratia 15:54–59
Eser P, Frotzler A, Zehnder Y, Schiessl H, Denoth J (2005) Assessment of anthropometric, systemic, and lifestyle factors influencing bone status in the legs of spinal cord injured individuals. Osteoporos Int 16:26–34
Eng JJ, Levins SM, Townson AF, Mah-Jones D, Bremner J, Huston G (2001) Use of prolonged standing for individuals with spinal cord injuries. Phys Ther 81:1392–1399
Kleerekoper M, Villanueva AR, Stanciu J, Rao DS, Parfitt AM (1985) The role of three-dimensional trabecular microstructure in the pathogenesis of vertebral compression fractures. Calcif Tissue Int 37:594–597
Acknowledgments
This study was supported by awards from the National Institutes of Health (R01NR010285, R01HD062507), the United States Department of Veterans Affairs, the Craig H. Neilsen Foundation, and by the Christopher Reeve Paralysis Foundation. The authors gratefully acknowledge the assistance of Andrew Littman PT, MA; Colleen McHenry MSE, Jason Wu MSE; Shih-Chiao Tseng PhD, PT; Elizabeth Faidley; Brandon Campbell; Deanna Frei, RT (R)(CT)(BD)(CBDT); April Miller, RTR; and Jered Sieren, BSRT(R) MR CT.
Conflicts of interest
The University of Iowa and Dr. Shields have intellectual property covered by a patent for technology used in this investigation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dudley-Javoroski, S., Saha, P.K., Liang, G. et al. High dose compressive loads attenuate bone mineral loss in humans with spinal cord injury. Osteoporos Int 23, 2335–2346 (2012). https://doi.org/10.1007/s00198-011-1879-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-011-1879-4