
Abstract
Objective
An investigation into the incidence of post-operative complications after thoracic surgery with 3 different physiotherapy masks.
Design
A prospective, consecutive, randomized comparison.
Setting
Department of Thoracic and Heart Surgery at a University Hospital. The treatments were performed by experienced and specially trained physiotherapists.
Patients
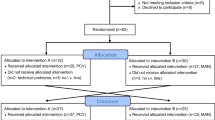
160 patients were evaluated. 60 patients undergoing heart surgery, 59 patients having pulmonary resection, and 41 patients with exploratory thoractomy.
Interventions
In each operative category the patients were treated with one of three face mask systems used in addition to routine chest physiotherapy. These were either continuous positive airway pressure (CPAP), positive expiratory pressure (PEP), or inspiratory resistance — positive expiratory pressure (IR-PEP).
Measurements and results
Post-operative pulmonary complications were assessed by forced vital capacity (FVC), arterial oxygen tension (PaO2), and chest X-ray examination, all measured pre-operatively and on the fourth and ninth post-operative day. The patients filled in a questionnaire expressing their opinion about their mask treatment. There was an equal decrease in FVC, FVC%, and PaO2, and equal frequency of atelectasis in the 3 mask treatments. More patients with the PEP mask favoured their system than did those with the other 2 systems.
Conclusion
There was no statistically significant difference between the treatments: continuous positive airway pressure (CPAP), positive expiratory pressure (PEP), and inspiratory resistance — positive expiratory pressure (IR-PEP) on post-operative complications. Any of the three treatments may be used as supplement to standard chest physiotherapy.
Similar content being viewed by others

References
Craig DB (1981) Postoperative recovery of pulmonary function. Anesth Analg 60:46–52
Froese AB, Bryan AC (1974) Effects of anesthesia and paralysis on diaphragmatic mechanics in man. Anesthesiology 41:242–255
Benhamou D, Samii K, Noviant Y (1983) Effect of analgesia on respiratory muscle function after upper abdominal surgery. Acta Anaesthesiol Scand 27:22–25
Martin RJ, Rogers RM, Gray BA (1980) The physiological basis for the use of mechanical aids to lung expansion. Am Rev Respir Dis 122:105–107
Ingwersen UM, Andersen JB (1992) Lungefysioterapi (Danish). Munksgaard, Copenhagen, pp 64–73
Dammann JF, McAslan TC (1977) Optimal flow pattern for mechanical ventilation of the lungs. Crit Care Med 5:128–136
Shapiro BA, Cane RD, Harrison RA (1984) Positive end-expiratory pressure therapy in adults with special reference to acute lung injury: A review of the literature and suggested clinical correlations. Crit Care Med 12:127–139
Duncan AW, Oh TE, Hillman DR (1986) PEEP and CPAP. Anaesth Intensive Care 14:236–250
Andersen JB, Olesen KP, Eikard B, Jansen E, Quist J (1980) Periodic continuous positive airway pressure, CPAP, by mask in the treatment of atelectasis. Eur J Respir Dis 61:20–25
Falk M, Kelstrup M, Andersen JB, Kinoshita T, Falk P, Støvring S, Gøthgen I (1984) Improving the ketchup bottle method with positive expiratory pressure, PEP. A controlled study in patients with cystic fibrosis. Eur J Respir Dis 65:423–432
Ricksten SE, Bengtsson A, Söderberg C, Thorden M, Kvist H (1986) Effects of periodic positive airway pressure by mask on postoperative pulmonary function. Chest 89:774–781
Roussos C (1985) Function and fatigue of respiratory muscles. Chest 88:124S-132S
Matthay MA, Wiener-Kronish JP (1989) Respiratory management after cardiac surgery., Chest 95:424–434
De Troyer A, Rosso J (1982) Reflex inhibition of the diaphragm by esophageal afferents. Neurosci Letters 30:43–46
Ford GT, Whitelaw WA, Rosenal TW, Cruse PJ, Guenter CA (1983) Diaphragm function after upper abdominal surgery in humans. Am Rev Respir Dis 127:431–436
Pasteur W (1910) Active lobar collapse of the lung after abdominal operations. Lancet X:1080–1083
Strandberg Å, Tokics L, Brismar B, Lundquist H, Hedenstierna G (1984) Atelectasis during anaesthesia and in the postoperative period. Acta Anesthesiol Scand 30:154–158
Ford GT, Guenter CA (1984) Toward prevention of postoperative pulmonary complications. Am Rev Respir Dis 130:4–5
Katz JA, Ozanne GM, Zinn SE, Fairly HB (1981) Time course and mechanisms of lung-volume increase with PEEP in acute pulmonary failure. Anesthesiology 54:9–16
Degn H, Haxholdt OS, Jørgensen BC, Krintel JJ, Risbo A (1986) Postoperative changes in pulmonary function. Pathological physiology, prophylaxis and treatment (Danish with English summary). Ugeskr Læger 148:2338–2341
Young MJ, Bresnitz EA, Strom BL (1983) Sample size nomograms for interpreting negative clinical studies. Ann Intern Med 99:248–251
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Ingwersen, U.M., Larsen, K.R., Bertelsen, M.T. et al. Three different mask physiotherapy regimens for prevention of post-operative pulmonary complications after heart and pulmonary surgery. Intensive Care Med 19, 294–298 (1993). https://doi.org/10.1007/BF01690551
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF01690551