
Abstract
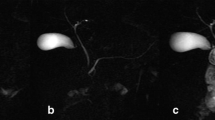
In the present study we compared sonographic measurements of the main pancreatic duct (MPD) following maximal secretin stimulation (75 CU intravenous in 1 min) in 15 chronic pancreatitis patients (CP) with those of 18 normal control subjects. The mean caliber of the main pancreatic duct was 1.2±0.4 mm in controls and 1.8±0.9 in patients with chronic pancreatitis (P<0.025). In the control group a dilatation of the duct with a peak at the third minute was found. In patients with chronic pancreatitis a flatter profile of the response curve with a slower increase and inconstant return to basal values was found. A statistically significant difference was found between absolute variations of MPD caliber over basal values (1.7±1.06 in controls vs 0.8±0.69 in CP, P<0.005) and the dilatation index [(D max -D)/D] (1.31±0.6 in controls vs 0.66±0.69 in CP, P<0.005). The mean percent increase at the third minute was 131% in control subjects vs 53% of patients with CP (P<0.0005). In the five cases of CP showing a caliber increase >100%, a persistent dilatation (100–200%) was found 15 min after secretin administration. At this time, the mean percent increase over basal value in controls was 25%. If we accept an abnormal response to secretin as evidence of pancreatic pathology, the absent or decreased (<50%) MPD dilatation after secretin and/or the persistence of a dilatation >100% at the 15 min, the sensitivity of this provocative test in discriminating early chronic pancreatitis from controls reaches the 86.6% (13 of 15 cases). Results of the present study suggest that the ultrasonographic examination of the main pancreatic duct (MPD) after maximal secretin stimulation may reveal morphological changes not visible under basal conditions, thus helping to diagnose early chronic pancreatitis (CP).
Similar content being viewed by others

References
Payan H, Sarles H, Demirdjian M, Gauthier AP, Cros RP, Durbec JP: Study of the histological features of chronic pancreatitis by correspondence analysis. Identification of chronic pancreatitis as an entity. Biomedicine 18:663–670, 1972
Sarles H, Sahel J, Staub JL, Bourry J, Langier R: Chronic pancreatitis.In: The Exocrine Pancreas. HT Howat, H Sarles (eds). London, WB Saunders, 179, p 402
Bolondi L, Gaiani S, Casanova P, Santi V, Labò G: Critical evaluation and controversial points of ultrasound findings in chronic pancreatitis.In Diagnostic Procedures in Pancreatic Disease. P Malfertheiner and H Ditschuneit (eds). Springer-Verlag, Berlin, pp 149–154
Bolondi L, Priori P, Gullo L, Santi V, Li Bassi S, Barbara L, Labò G: Relationship between morphological changes detected by ultrasonography and pancreatic exocrine function in chronic pancreatitis. Pancreas 2:222–229, 1987
Bolondi L, Gaiani S, Gullo L, Labò G: Secretin administration induces a dilatation of main pancreatic duct. Dig Dis Sci 29:802–808, 1984
Gullo L, Costa PL, Fontana G, Labò G: Investigation of exocrine pancreatic function by continuous infusion of cerulein and secretin in normal subjects and in chronic pancreatitis. Digestion 14:97–107, 1976
Parulekar SG: Ultrasonic evaluation of the pancreatic duct. J Clin Ultrasound 8:457–463, 1980
Hadidi A: Pancreatic duct diameter: Sonographic measurement in normal subjects. J Clin Ultrasound 11:17–22, 1983
Blangy S, Cornud F, Sibert A, Benacerraf R: Etude du canal de Wirsung normal en échographie temps réel. Confrontation avec cathétérisme rétrograde. J Radiol 65:35–39, 1984
Masoero G, Bianco A, Colaferro S, Marchetto M, Rossanino A, Marucci M: Ultrasonic evaluation of Wirsung (W) after hormonal stimulations in controls and in patients with chronic pancreatitis. Ital J Gastroenterol 18:243(A), 1986
Glaser J, Hagemann B, Krummenerl T, Schneider M, Hultsch E, van Husen N, Gerlach U: Sonographic imaging of the pancreactic duct. New diagnostic possibilities using secretin stimulation. Dig Dis Sci 32(10):1075–1081, 1987
Glaser J, Esser W, Holtmannspotter K: Sonographische Darstellung des Pankreasganges vor und nach Sekretinstimulation: hilfreich in der Diagnose der chronischen Pankreatitis. Ultraschall 6:106–109, 1985
Cotton B: Endoscopic retrograde pancreatography.In The Exocrine Pancreas. HT Howat, H Sarles (eds). WB Saunders, 1979, pp 278–298
Kizu M, Newman J, Cotton B, Kasugai T: Histological correlation with pancreatography in necropsy specimens. Gut 18:339–340, 1977
Kasugai T, Kuno N, Kizu M: Manometric endoscopic retrograde pancreatocholangiography. Techniques, significance and evaluation. Am J Dig Dis 19:485–502, 1974
Niederau C, Grendell J: Diagnosis of chronic pancreatitis. Gastroenterology 88:1973–1995, 1985
Karasawa E, Goldberg HI, Moss AA, Federle MP, London SS: CT pancreatogram in carcinoma of the pancreas and chronic pancreatitis. Radiology 148:489–493, 1983
Callen PW, London SS, Moss AA: Computed tomographic evaluation of the dilated pancreatic duct. Radiology 134:253–255, 1980
Foley WD, Stewart ET, Lawson TL, Geenan J, Loguidice J, Maher L, Unger J: Computed tomography, ultrasonography, and endoscopic retrograde cholangiopancreatography in the diagnosis of pancreatic disease: a comparative study. Gastrointest Radiol 5:29–35, 1980
Ferrucci JT Jr, Wittemberg J, Black EB, Kirkpatrick RH, Hall DA: Computed body tomography in chronic pancreatitis. Radiology 130:175–182, 1979
Simeone JF, Edelman RR, Stark DD, Wittemberg J, White EM, Butch RJ, Mueller PR, Brady TJ, Ferrucci JT Jr: Surface coil MR imaging of abdominal viscera. Part III. The Pancreas Radiology 157:437–441, 1985
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bolondi, L., Li Bassi, S., Gaiani, S. et al. Impaired response of main pancreatic duct to secretin stimulation in early chronic pancreatitis. Digest Dis Sci 34, 834–840 (1989). https://doi.org/10.1007/BF01540267
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01540267