Abstract
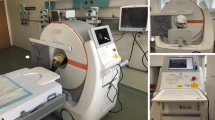
This study reviews the initial clinical experience using a portable computed tomographic (CT) scanner in the trauma resuscitation unit (TRU), intensive care units (ICUs), and operating rooms (ORs) of a large trauma center. Data were collected on the first 200 patients scanned within the trauma center (including 92 in the TRU, 92 in the ICUs, and 16 in the ORs) over the first 5 months of operation. Evaluation forms were completed by interpreting radiologists, CT technicians operating the system, and nurses/clinicians involved with patients being scanned. Information sought included subjective image quality, ease of use, software and hardware limitations, accessibility to and monitoring of patients during scanning, mobility, and perceived advantages or limitations compared to fixed CT. Radiation scatter also was measured to determine the safety of the scanner for portable use.
CT scans of 224 body regions performed in 200 patients included: cranium (163), cervical spine (21), abdomen/pelvis (14), chest (12), face (8), thoracic/lumbar spine (4), and temporal bone (2). Image quality was judged subjectively as excellent (107), good (99), poor (6), or artifact degraded (12). Patient transfer to the scanner was judged to be easy (63) or fair/difficult (4). Patient accessibility and monitoring during scanning was assessed as easy (61) or fair/difficult (6). Access in the smaller TRU bays was more difficult than in the ICU or OR. Cited advantages over fixed CT included decreased risk and cost of transport, quicker assessment of cranial injury on admission, and more rapid postcraniotomy assessment. Limitations cited were relatively slow scan speed, slightly poorer image quality, and technical limits on scanning multiple body regions. Radiation scatter was 25% of the ALARA (as low as reasonably achievable) target for the scanner operator. Initial clinical experience with mobile CT in the TRU, ICU, and OR of a major trauma center shows application for focused admission scanning, assessment of critically ill ICU patients, and immediate postoperative assessment after craniotomy. The system has been incorporated easily into the trauma center and has been accepted enthusiastically. Further technical improvements are anticipated to extend the range of applications in this clinical setting.
Article PDF
Similar content being viewed by others


References
Bramen SS, Dunn SM, Amico CA, Millman RP. Complications of intrahospital transport in critically ill patients. Ann Intern Med 1987;107:469–73.
Smith I, Fleming S, Cernaianu A. Mishaps during transport from the intensive care unit. Crit Care Med 1990;18:278–81.
Andrews PJD, Piper IR, Dearden NM, Miller JD. Secondary insults during intrahospital transport of head-injured patients. Lancet 1990;335:327–30.
Weg JG, Haas CF: Safe intrahospital transport of critically ill ventilator-dependent patients. Chest 1989;96:631–5.
Indeck M, Peterson S, Smith J, Brotman S. Risk, cost, and benefit of transporting ICU patients for special studies. J Trauma 1988;28:1020–5.
Hurst JM, Davis K Jr, Johnson DJ, Branson RD, Campbell RS, Branson PS. Cost and complications during in-hospital transport of critically-ill patients: a prospective cohort study. J Trauma 1990;33:582–5.
Alvarez-Sabin J, Turon A, Lozano-Sanchez M, Vasquez J, Codina A. Delayed posttraumatic hemorrhage “Spat-Apoplexie”. Stroke 1995;26:1531–5.
Stein SC, Spettell C, Young G, Ross SE. Delayed and progressive brain injury in closed-head trauma: radiologic demonstration. Neurosurgery 1993;32:25–31.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Mirvis, S.E., Shanmuganathan, K., Donohue, R. et al. Mobile computed tomography in the trauma/critical care environment: Preliminary clinical experience. Emergency Radiology 4, 212–217 (1997). https://doi.org/10.1007/BF01508173
Issue Date:
DOI: https://doi.org/10.1007/BF01508173