
Abstract
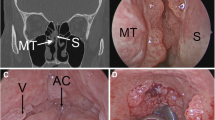
A 23 year old male presented to the Otolaryngology clinic with 6 months of hoarseness and poor voice projection without improvement from speech therapy or medical anti-reflux medication. Upon examination he was found to have multiple polypoid lesions emanating from bilateral false vocal folds, left true vocal fold, and the anterior commissure. Biopsy and potassium titanyl phosphate (KTP) laser ablation with bevacizumab injection provided treatment and confirmed the clinical suspicion of squamous cell papilloma. Despite 3 years of treatment, the papillomatosis proved difficult to control, requiring a procedure approximately every 3 months. In an attempt to control the course of the disease the patient received a series of three bevacizumab and three cidofovir injections. Serial biopsies showed mild atypia within the squamous cell papillomas. Two separate biopsies confirmed presence of human papillomavirus (HPV) 6/11 via in situ hybridization with appropriate controls. There is promising research that the quadrivalent HPV (types 6, 11, 16, and 18) vaccine both reduces the disease burden in patients with active disease and reduces the incidence of recurrent respiratory papillomatosis (RRP). Other studies have shown that local immunologic dysregulation may play a role in RRP pathogenesis. Therefore new treatment options, to include PDL-1 blockade, offer hope in treating this benign condition with high morbidity and rare mortality.




Similar content being viewed by others


References
Omland T, Akre H, Lie KA, Jebsen P, Sandvik L, Brøndbo K. Risk factors for aggressive recurrent respiratory papillomatosis in adults and juveniles. PLoS ONE. 2014;9(11):e113584.
Chirilă M, Bolboacă SD. Clinical efficiency of quadrivalent HPV (types 6/11/16/18) vaccine in patients with recurrent respiratory papillomatosis. Eur Arch Otorhinolaryngol. 2014;271(5):1135–42.
Richardson M, Gale N, Hille J, Zidar N. Squamous cell papilloma and squamous cell papillomatosis. In: Chan JKC, Grandis JR, Takashi T, Slootweg PJ, El-Nagger AK, editors. WHO classification of head and neck tumours. Lyon: International Agency for Research on Cancer; 2017.
Dickens P, Srivastava G, Loke SL, Larkin S. Human papillomavirus 6, 11, and 16 in laryngeal papillomas. J Pathol. 1991;165(3):243–6.
Wiatrak BJ, Wiatrak DW, Broker TR, Lewis L. Recurrent respiratory papillomatosis: a longitudinal study comparing severity associated with human papilloma viral types 6 and 11 and other risk factors in a large pediatric population. Laryngoscope. 2004;114(11 Pt 2 Suppl 104):1–23.
Ruiz R, Achlatis S, Verma A, Born H, Kapadia F, Fang Y, Pitman M, Sulica L, Branski RC, Amin MR. Risk factors for adult-onset recurrent respiratory papillomatosis. Laryngoscope. 2014;124:2338–44.
Silverberg MJ, Thorsen P, Lindeberg H, Grant LA, Shah KV. Condyloma in pregnancy is strongly predictive of juvenile-onset recurrent respiratory papillomatosis. Obstet Gynecol. 2003;101(4):645–52.
Karatayli-Ozgursoy S, Bishop JA, Hillel A, Akst L, Best SR. Risk factors for dysplasia in recurrent respiratory papillomatosis in an adult and pediatric population. Ann Otol Rhinol Laryngol. 2016;125(3):235–41.
Aslanzadeh J. Preventing PCR amplification carryover contamination in a clinical laboratory. Ann Clin Lab Sci. 2004;34(4):389–96.
Papaioannou VA, Lux A, Voigt-Zimmermann S, Arens C. Treatment outcomes of recurrent respiratory papillomatosis: retrospective analysis of juvenile and adult cases. HNO. 2018;66(Suppl 1):7–15.
Novakovic D, Cheng ATL, Zurynski Y, Booy R, Walker PJ, Berkowitz R, Harrison H, Black R, Perry C, Vijayasekaran S, Wabnitz D, Burns H, Tabrizi SN, Garland SM, Elliott E, Brotherton JML. A prospective study of the incidence of juvenile-onset recurrent respiratory papillomatosis after implementation of a national HPV vaccination program. J Infect Dis. 2018;217(2):208–12.
Villa LL, Ault KA, Giuliano AR, Costa RL, Petta CA, Andrade RP, Brown DR, Ferenczy A, Harper DM, Koutsky LA, Kurman RJ, Lehtinen M, Malm C, Olsson SE, Ronnett BM, Skjeldestad FE, Steinwall M, Stoler MH, Wheeler CM, Taddeo FJ, Yu J, Lupinacci L, Railkar R. Immunologic responses following administration of a vaccine targeting human papillomavirus Types 6, 11, 16, and 18. Vaccine. 2006;24(27–28):5571–83.
Makiyama K, Hirai R, Matsuzaki H. Gardasil vaccination for recurrent laryngeal papillomatosis in adult men: first report: changes in HPV antibody titer. J Voice. 2017;31(1):104–6.
Gi RETP., San Giorgi MR, Pawlita M, Michel A, van Hemel BM, Schuuring EM, van den Heuvel ER, van der Laan BF, Dikkers FG. Immunological response to quadrivalent HPV vaccine in treatment of recurrent respiratory papillomatosis. Eur Arch Otorhinolaryngol. 2016;273(10):3231–6.
Lucs AV, DeVoti JA, Hatam L, Afzal A, Abramson AL, Steinberg BM, Bonagura VR. Immune dysregulation in patients persistently infected with human papillomaviruses 6 and 11. J Clin Med. 2015;4(3):375–88.
Ahn J, Bishop JA, Roden RBS, Allen CT, Best SRA. The PD-1 and PD-L1 pathway in recurrent respiratory papillomatosis. Laryngoscope. 2018;128(1):E27–E32.
Liu T, Greenberg M, Wentland C, Sepe B, Bowe S, Diercks G, Huynh T, Mino-Kenudson M, Schlegel R, Kodack D, Benes C, Engelman J, Hartnick C. PD-L1 expression and CD8 + infiltration shows heterogeneity in juvenile recurrent respiratory papillomatosis. Int J Pediatr Otorhinolaryngol. 2017;95:133–8.
Author information
Authors and Affiliations
Corresponding author
Additional information
Disclaimer
The opinions and assertions expressed herein are those of the author and are not to be construed as official or representing the views of the Department of the Navy or the Department of Defense.
Rights and permissions
About this article

Cite this article
Bentley, P.L., Coulter, M.J. & Nelson, B.L. Squamous Cell Papillomatosis in the Setting of Recurrent Respiratory Papillomatosis. Head and Neck Pathol 13, 235–238 (2019). https://doi.org/10.1007/s12105-018-0912-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12105-018-0912-8